The TMJ & Airway Connection
Why the jaw and the upper airway are evaluated together in TMJ care — the anatomy that links bite, mandibular position, snoring, and obstructive sleep apnea, and how a single oral appliance can sometimes address both. From Dr. Yolanda Cruz's TMJ-focused dental practice on the PATH in downtown Toronto.
The jaw and the airway are closely related anatomically — the position of the lower jaw influences, in part, how open or restricted the upper airway is. When the mandible is positioned further back than its optimal alignment because of bite issues, muscle tension, or structural factors, the tongue and soft tissues of the throat may also shift backward, reducing the space available for airflow. This is one reason why patients with temporomandibular disorder (TMD) may have a higher rate of sleep-disordered breathing, including snoring and obstructive sleep apnea. The relationship also works in the other direction: disrupted sleep and the physiological effects of repeated airway obstruction can increase the sensitivity of the central nervous system — a process called central sensitization — which may amplify the perception of pain and make TMD symptoms more persistent. Dr. Yolanda Cruz evaluates patients for both TMD and sleep-disordered breathing as part of a comprehensive assessment, and in some cases a single custom oral appliance can help address both concerns simultaneously. Book a TMJ & airway assessment in downtown Toronto.
How jaw position affects the airway
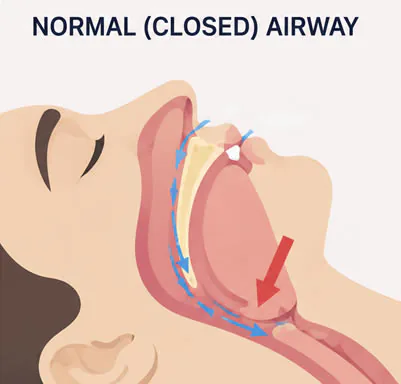
The lower jaw, the tongue, and the soft tissues of the throat are mechanically linked. When the mandible is positioned further back than its optimal alignment — because of bite issues, muscle tension, or structural factors — the tongue and the soft tissues of the throat may also shift backward, reducing the space available for airflow.
A small reduction in upper-airway diameter during the day is usually compensated for. The same reduction during sleep — when muscle tone falls and the patient is lying flat — can be the difference between quiet breathing, snoring, and frank obstructive episodes.
Reviewed by Dr. Yolanda Cruz, DDS · Dr. Yolanda Cruz Dentistry On The Path · Toronto, ON

Why TMD patients have a higher rate of snoring and obstructive sleep apnea
Because mandibular position influences upper-airway dimensions, the same anatomical and muscular factors that contribute to TMD — a posteriorly displaced mandible, clenched and over-tonic masticatory muscles, forward head posture, skeletal asymmetries — can also reduce the airway during sleep.
This is one reason why patients with temporomandibular disorder (TMD) may have a higher rate of sleep-disordered breathing, including snoring and obstructive sleep apnea. It also explains why a patient who comes in for jaw pain may, on careful history, also describe loud snoring, morning headaches, or unrefreshing sleep — symptoms that point upstream to the same anatomical problem.
For an overview of the sleep-apnea side of the picture, see What is sleep apnea? and the STOP-BANG risk questionnaire.
How bruxism and clenching fit into the picture
Bruxism — nocturnal teeth grinding and clenching — is one of the most common contributors to TMD, and there is now a substantial body of evidence linking sleep bruxism to disordered breathing during sleep. For many patients, the grinding is not an isolated habit; it is part of the body's response to repeated micro-arousals from airway events. The jaw muscles activate, the mandible is pulled forward, and the airway is — briefly — reopened.
That is useful in the short term and damaging in the long term: it produces the worn enamel, the cracked restorations, the temporal headaches, and the masseter hypertrophy that bring patients in for TMJ care. See oral appliances and sleep tips for snoring & sleep apnea for the related self-care and treatment pages.
The anatomy that links the TMJ and the upper airway
Several anatomical structures sit at the crossroads of bite, jaw, and airway. When any of them is out of balance, the effect is felt at both ends.
The mandible
The lower jaw. Its forward-backward position is one of the strongest mechanical determinants of how much space is available behind the tongue.
The tongue
Anchored to the floor of the mouth and the front of the mandible. When the jaw shifts back, the tongue follows — reducing the space at the back of the throat.
The soft tissues of the throat
The soft palate, uvula, and pharyngeal walls. These collapse most easily during sleep, particularly when muscle tone falls and the patient is lying flat.
The masticatory muscles
The masseter, temporalis, and pterygoids power chewing and clenching. They are overactive in TMD and in sleep bruxism associated with airway events.
The temporomandibular joint
Two paired joints in front of each ear. Joint position, disc position, and the way the joint loads during sleep all influence where the mandible sits.
Posture & cervical alignment
Forward head posture pulls the mandible back and the hyoid down, narrowing the airway. Posture is a shared contributor to TMD and to sleep-disordered breathing.
Central sensitization — why airway problems can make TMD pain worse
The relationship also works in the other direction. Disrupted sleep and the physiological effects of repeated airway obstruction can increase the sensitivity of the central nervous system, a process called central sensitization, which may amplify the perception of pain and make TMD symptoms more persistent.
Clinically, this means a patient whose TMD symptoms have plateaued or are unusually hard to settle — despite an appliance, despite Botox, despite a sound treatment plan — should be evaluated for an unrecognized sleep-breathing problem. Treating the airway can be what allows the jaw pain to finally respond.
This is also why the practice's diagnostic process — see your visit & diagnostic process and TMJ/TMD diagnostic technology — routinely asks about sleep quality, snoring, witnessed apneas, morning headaches, and daytime fatigue, not just about the jaw.
Warning signs that the jaw and the airway are connected in your case
If you recognize several of the following together, the evaluation should look at both TMJ and sleep-disordered breathing — not one in isolation:
- Jaw pain, jaw clicking, or limited opening alongside snoring or witnessed breathing pauses
- Morning headaches, especially across the temples or at the base of the skull
- Worn or chipped teeth, cracked restorations, masseter hypertrophy (visibly enlarged jaw muscles)
- Waking unrefreshed despite seven or more hours in bed
- Daytime fatigue, brain fog, or difficulty concentrating
- A bed partner who reports loud snoring or pauses in breathing
- TMD symptoms that have plateaued or that flare badly after poor sleep
- A small or recessed lower jaw on facial profile, or a high-vaulted narrow palate
None of these is, on its own, diagnostic — but the pattern matters. If you recognize several of them, a thorough evaluation can help identify whether the jaw and the airway are contributing to your symptoms.

Because of this relationship, both are evaluated together
Because of the anatomical and physiological links between TMD and sleep-disordered breathing, Dr. Yolanda Cruz evaluates patients for both as part of a comprehensive assessment. The history asks about jaw symptoms and sleep quality, snoring, witnessed apneas, morning headaches, and daytime fatigue.
The clinical examination looks at bite and jaw mechanics, masticatory-muscle tone, joint sounds, range of motion, the position of the mandible at rest, and the visible architecture of the soft palate, tonsils, and tongue. Where indicated, 3D CBCT imaging is used to visualize the joints, the condyles, and the upper-airway dimensions, and T-Scan or Joint Vibration Analysis is used to characterize the bite and the joint.
When sleep-disordered breathing is suspected, a referral for a home sleep test or in-lab polysomnography is arranged so that any oral-appliance therapy is grounded in a proper sleep diagnosis — not assumed.

When a single custom appliance can address both
In some cases, a single custom oral appliance can help address both concerns simultaneously. Mandibular-advancement designs hold the lower jaw slightly forward during sleep, which both protects the joint from overloading and increases the cross-sectional area of the upper airway — reducing snoring and, in mild to moderate obstructive sleep apnea, reducing apnea-hypopnea events.
Whether this approach is appropriate depends on the joint examination, the bite, the patient's sleep-test results, and an honest conversation about goals. Some patients are better served by a TMJ-focused stabilization splint plus separate CPAP for the airway; some by a combined device; some by a referral to an oral & maxillofacial surgeon or sleep physician. The point of the comprehensive evaluation is to be able to tell those situations apart.
For the related treatment pages, see oral appliances, the TMJ stabilization appliance, and the sleep apnea treatment overview.
Dr. Cruz's clinical note
"In my experience, the patients whose TMJ symptoms are hardest to settle are very often the patients with an unrecognized airway problem at night. The jaw isn't a closed system — it sits at the front of an airway that has to stay open every minute of the night. If we treat the jaw without ever looking upstream at the airway, we sometimes get short-term relief, and we sometimes spend months trying to figure out why the same symptoms keep coming back."
"That is why the consultation always asks about sleep, snoring, morning headaches, and daytime fatigue alongside the jaw. It is not because every TMJ patient has obstructive sleep apnea — many don't. It is because we cannot tell which patient does and which patient doesn't unless we ask, examine, and image properly. Once we know, the treatment plan is much more honest."
— Dr. Yolanda Cruz, DDS, Dr. Yolanda Cruz Dentistry On The Path, Downtown Toronto
Frequently asked questions about the TMJ & airway connection
The jaw and the upper airway are mechanically linked: the position of the lower jaw influences, in part, how open or restricted the upper airway is. When the mandible is positioned further back than its optimal alignment because of bite issues, muscle tension, or structural factors, the tongue and the soft tissues of the throat may also shift backward, reducing the space available for airflow. The same factors that contribute to TMD therefore also tend to contribute to sleep-disordered breathing — which is why both are evaluated together at this practice.
Yes — this is one reason patients with temporomandibular disorder (TMD) may have a higher rate of sleep-disordered breathing, including snoring and obstructive sleep apnea. Because mandibular position influences upper-airway dimensions, the same anatomical and muscular factors that contribute to TMD — a posteriorly displaced mandible, clenched and over-tonic masticatory muscles, forward head posture, skeletal asymmetries — can also reduce the airway during sleep. This is why a TMD history at this practice routinely also asks about snoring, witnessed breathing pauses, and morning headaches. See What is sleep apnea?
The relationship between the jaw and the airway works in both directions. Disrupted sleep and the physiological effects of repeated airway obstruction can increase the sensitivity of the central nervous system — a process called central sensitization — which may amplify the perception of pain and make TMD symptoms more persistent. In practice this means a patient whose TMD has plateaued despite a sound treatment plan should be evaluated for an unrecognized sleep-breathing problem; treating the airway can be what finally allows the jaw pain to settle.
In some cases, yes — a single custom oral appliance can help address both concerns simultaneously. Mandibular-advancement designs hold the lower jaw slightly forward during sleep, which both protects the joint from overloading and increases the cross-sectional area of the upper airway, reducing snoring and (in mild to moderate obstructive sleep apnea) reducing breathing events. Whether a combined approach is right for you depends on the joint examination, the bite, your sleep-test results, and your goals. Some patients are better served by a TMJ stabilization splint plus separate CPAP. See oral appliances.
Often, yes — particularly if your history, examination, or imaging suggests airway involvement. Where sleep-disordered breathing is suspected, a home sleep test or in-lab polysomnography is arranged so that any oral-appliance therapy is grounded in a proper sleep diagnosis rather than assumed. Without that diagnostic step, it is impossible to know whether an appliance is doing what you actually need it to do for the airway. See the STOP-BANG risk questionnaire.
If you experience jaw pain, headaches, clenching, snoring, or poor-quality sleep, these issues may be connected. A thorough evaluation can help identify whether the jaw and the airway are contributing to your symptoms. Other prompts: jaw discomfort with witnessed breathing pauses, morning headaches with worn or chipped teeth, TMD symptoms that worsen after a bad night's sleep, or a bed partner who reports loud snoring. Book a TMJ & airway assessment or call 416-595-5490.
Medical Disclaimer
This content is for informational purposes only and does not constitute dental or medical advice, diagnosis, or treatment. The relationship between TMJ disorders and sleep-disordered breathing varies by individual; diagnosis of obstructive sleep apnea requires a sleep test interpreted by a qualified sleep physician, and oral-appliance therapy is one option among several. Some cases require referral to a sleep physician, an oral and maxillofacial surgeon, or another specialist. Consult Dr. Yolanda Cruz or another qualified dental or medical professional regarding your symptoms and treatment options. Individual results may vary.
Book a TMJ & airway assessment in Toronto
If you are experiencing jaw discomfort, facial tension, clicking, headaches, snoring, or sleep-related concerns, Dr. Cruz's team can help assess the underlying factors and discuss appropriate treatment options.