What Is Sleep Apnea?
A clinical introduction to obstructive sleep apnea (OSA), how it differs from snoring, why it so often goes undiagnosed, and the role a TMJ & airway-focused dentist plays alongside your sleep physician. From Dr. Yolanda Cruz's PATH-level practice in downtown Toronto.
Sleep is a biological necessity, and when it is repeatedly disrupted, the consequences extend well beyond tiredness. Obstructive sleep apnea (OSA) is the most prevalent form of sleep-disordered breathing in Canada, and many cases go undiagnosed. As a general dentist with a focused practice in TMJ and sleep-disordered breathing, Dr. Cruz can evaluate patients for signs of sleep-disordered breathing, provide oral appliance therapy where indicated, and work collaboratively with sleep physicians to support appropriate diagnosis and care.
What is sleep apnea?
Sleep apnea is characterized by repeated interruptions to breathing during sleep. There are three recognized types, distinguished by what causes the breathing to stop and how the body responds.
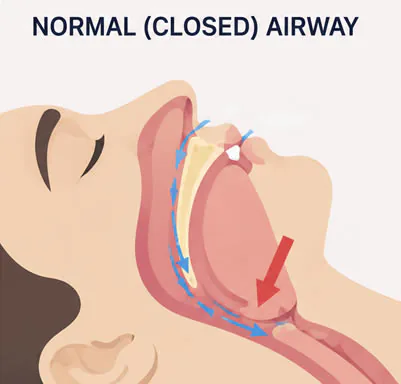
The most common form — obstructive sleep apnea, or OSA — occurs when the muscles and soft tissues of the upper airway relax during sleep to the point that the airway partially or completely collapses. Breathing stops, blood oxygen levels drop, and the body briefly arouses, often without the person’s awareness. This cycle can repeat many times per night.
Reviewed by Dr. Yolanda Cruz, DDS · Dr. Yolanda Cruz Dentistry On The Path · Toronto, ON
Three recognized types of sleep apnea
Distinguishing between these is essential because the underlying mechanism determines what treatment options are appropriate — in particular, whether oral appliance therapy is even on the table.
Obstructive sleep apnea (OSA)
The most common form. The muscles and soft tissues of the upper airway relax during sleep to the point that the airway partially or completely collapses. Contributing factors include jaw position, tongue posture, airway anatomy, weight, and hormonal status.
Central sleep apnea
A neurological form in which the brain does not send appropriate signals to the breathing muscles. The airway itself is not blocked, but the drive to breathe is absent. This type does not respond to oral appliance therapy and requires medical management.
Mixed / complex sleep apnea
A combination of obstructive and central events. Oral appliances may be considered in select cases, under the guidance of a sleep physician.
Key terms
If you've been told you may have sleep apnea, or you've had a sleep study, these are the terms that will come up most often.
- Apnea: A complete cessation of airflow lasting 10 seconds or more.
- Hypopnea: A partial reduction in airflow accompanied by a measurable drop in blood oxygen levels.
- AHI (Apnea-Hypopnea Index): The total number of apnea and hypopnea events per hour of sleep — used to classify severity.
OSA severity classification
According to the American Academy of Sleep Medicine, OSA severity in adults is classified by the AHI score:
| AHI (Events Per Hour) | Classification |
|---|---|
| 0 – 5 | Normal (adult) |
| 5 – 15 | Mild OSA |
| 15 – 30 | Moderate OSA |
| 30+ | Severe OSA |

OSA in children
Children should not snore regularly. In the pediatric population, enlarged tonsils and adenoids are the most common cause of sleep-disordered breathing.
Untreated childhood OSA has been associated with behavioural difficulties, impaired growth and development, altered craniofacial growth, and bedwetting. These are not subtle long-term effects — they show up in the school years and can persist.
If your child snores regularly beyond the duration of a cold, early assessment is recommended. A combined evaluation between your child's physician and a dentist familiar with airway and craniofacial growth can help identify whether further investigation is warranted.
Snoring vs. obstructive sleep apnea
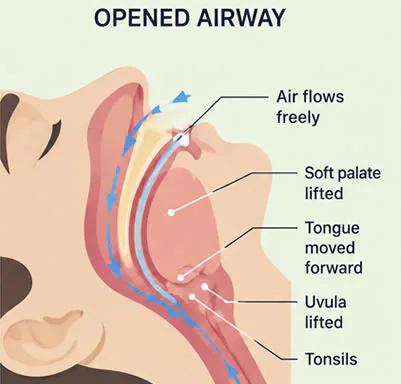
Snoring occurs when the soft tissues of the throat — including the soft palate, the uvula, and surrounding structures — vibrate as air passes through a narrowed airway during sleep.
Snoring and sleep apnea are not the same condition. Not everyone who snores has sleep apnea. However, many people with OSA do snore, and some individuals with what appears to be simple snoring are experiencing significant airway obstruction without being aware of it.
In children, snoring should always be assessed promptly, as it is not considered a normal finding. In adults, persistent snoring — especially when accompanied by any of the warning signs below — is worth investigating.
Signs that snoring may warrant further evaluation
If you or a family member snores and any of the following are also present, an evaluation can help determine whether further investigation is appropriate:
- Gasping, choking, or snorting sounds during sleep
- Witnessed pauses in breathing reported by a bed partner
- Waking unrefreshed despite a full night's sleep
- Significant daytime sleepiness
- Morning headaches or jaw pain
- Frequent nighttime urination
- Mood changes or difficulty concentrating
Health risks associated with untreated sleep apnea
Untreated obstructive sleep apnea is associated with a number of serious health conditions. The information below reflects findings from published medical research.
Cardiovascular
Repeated drops in blood oxygen place strain on the cardiovascular system. Untreated OSA is associated with hypertension, increased risk of heart attack, stroke, and cardiac arrhythmia.
Metabolic
OSA has been linked to insulin resistance, type 2 diabetes, and weight gain. Disrupted sleep also affects hormones that regulate appetite.
Cognitive & psychological
Chronic sleep fragmentation can impair memory, concentration, and executive function. Depression and anxiety occur more frequently in people with untreated OSA.
Safety
Research indicates that people with untreated OSA are at significantly elevated risk of motor vehicle accidents due to daytime sleepiness. Workplace accident risk is also increased.
Relationships
The disruption that snoring and restless sleep cause to household members is a real and frequently reported consequence of untreated sleep-disordered breathing.
Daytime function
Even where the strict medical risks have not yet developed, untreated OSA shows up as chronic fatigue, low energy, and reduced quality of life. Many patients only realise how compromised they were once treatment begins.

The role of the dentist in sleep apnea
Sleep apnea is a medical condition. Diagnosis is made by a sleep physician, normally on the basis of a sleep study and a clinical assessment.
The dentist's role is complementary. In a TMJ and airway-focused practice, the dentist can:
- Recognise dental and craniofacial signs that suggest sleep-disordered breathing (worn dentition, scalloped tongue, narrow palate, recessed lower jaw)
- Take a focused symptom history and screen with validated tools such as STOP-BANG
- Refer to a sleep physician where investigation is warranted
- Provide oral appliance therapy where the patient is diagnosed with OSA and the physician has determined that an appliance is appropriate
- Manage TMJ symptoms that frequently coexist with airway problems
To go deeper, see sleep apnea treatment, oral appliances, and the TMJ-airway connection.
Frequently asked questions about sleep apnea
Obstructive sleep apnea is the most common form of sleep apnea, in which the muscles and soft tissues of the upper airway relax during sleep to the point that the airway partially or completely collapses. Breathing stops, blood oxygen levels drop, and the body briefly arouses — often without the person's awareness. This cycle can repeat many times per night. Contributing factors include jaw position, tongue posture, airway anatomy, weight, and hormonal status.
Snoring is the sound of soft-tissue vibration in a narrowed airway; sleep apnea is repeated cessation of breathing during sleep. Many people who snore do not have sleep apnea, and many people with sleep apnea do snore. However, some patients who appear to be "just snoring" are in fact having significant airway obstruction events without realising it. Gasping, choking, witnessed pauses, morning headaches, and daytime sleepiness alongside snoring all suggest the situation should be evaluated.
Sleep apnea is a medical condition and diagnosis must be made by a physician, typically a sleep specialist. Diagnosis is made on the basis of a sleep study — either in-lab polysomnography or a home sleep apnea test — which generates the AHI (Apnea-Hypopnea Index). The AHI is used to classify the disorder as mild (5–15), moderate (15–30), or severe (30+). A dentist does not diagnose sleep apnea, but a TMJ-focused dental practice can screen, refer, and provide oral appliance therapy where appropriate after diagnosis.
Published medical research links untreated obstructive sleep apnea to hypertension, increased risk of heart attack, stroke, cardiac arrhythmia, insulin resistance, type 2 diabetes, and weight gain. It is also associated with impaired memory, concentration, and executive function, increased rates of depression and anxiety, and significantly elevated risk of motor vehicle and workplace accidents due to daytime sleepiness. The household-relationship impact of snoring and restless sleep is also a real and frequently reported consequence.
Yes. Children should not snore regularly — in the pediatric population, enlarged tonsils and adenoids are the most common cause of sleep-disordered breathing. Untreated childhood OSA has been associated with behavioural difficulties, impaired growth and development, altered craniofacial growth, and bedwetting. If a child snores regularly beyond the duration of a cold, early assessment is recommended. A combined evaluation involving the child's physician and a dentist familiar with airway and craniofacial growth can help identify whether further investigation is needed.
A dentist with focused training in TMJ and sleep-disordered breathing can screen for signs of OSA, refer to a sleep physician where investigation is warranted, and — once a diagnosis is in place — provide custom oral appliance therapy where the physician has determined an appliance is appropriate. The dentist also manages TMJ symptoms that frequently coexist with airway problems. See sleep apnea treatment and oral appliances for how that works in practice, or book a screening consultation with Dr. Cruz on the PATH in downtown Toronto.
Medical Disclaimer
This content is for informational purposes only and does not constitute dental or medical advice, diagnosis, or treatment. Sleep apnea is a medical condition and diagnosis must be made by a physician. Treatment outcomes and the appropriateness of oral appliance therapy vary by individual and depend on the type and severity of the underlying sleep-disordered breathing. Consult Dr. Yolanda Cruz or another qualified dental professional, alongside your physician, regarding your symptoms and treatment options. Individual results may vary.
Concerned about your sleep, snoring, or daytime fatigue?
Book a screening consultation with Dr. Cruz. You'll leave with a clear picture of whether your symptoms warrant referral for a sleep study — and what dental treatment options may be available once a diagnosis is in place.