Managing the Arthritic TMJ in Downtown Toronto
Conservative, joint-protective care for arthritic changes in the temporomandibular joint — supporting natural adaptation, the pseudodisc process, and long-term comfortable function. Provided by Dr. Yolanda Cruz at the office on the PATH at Bay & Queen.
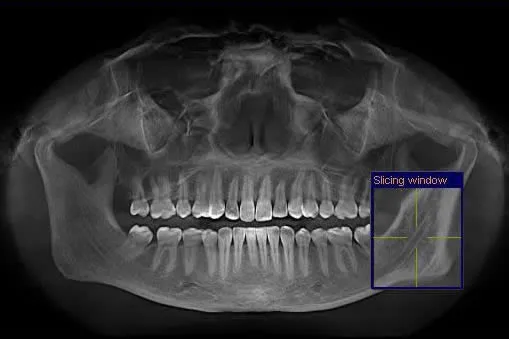
An "arthritic" temporomandibular joint sounds frightening — but in most cases it is not a sentence of chronic pain. When the TMJ disc has been displaced for a long time, the joint remodels: bone surfaces flatten, small spurs (osteophytes) may form, and the contour of the condyle changes. On CBCT imaging this remodeling meets the radiographic definition of arthritis, but many patients with these findings have little or no symptoms — the joint has adapted. Dr. Yolanda Cruz manages arthritic TMJ presentations conservatively, within the scope of general dentistry, with the goal of supporting the natural adaptation process. Schedule an evaluation or call 416-595-5490.
What "arthritic TMJ" really means
When a TMJ disc has been displaced for a long period of time, the jaw joint begins to remodel. The bony surfaces of the condyle and the glenoid fossa change shape in response to the altered mechanics. On imaging, this remodeling may appear as bone spurs (osteophytes), flattening of the condylar head, sclerosis, erosions, or surface irregularities — findings that technically meet the radiographic definition of osteoarthritis of the TMJ.
This can sound alarming, but it is important to understand that these radiographic changes do not necessarily mean ongoing pain, locking, or permanent disability. Many people have arthritic-looking TMJs on CBCT and function comfortably day to day. The joint has a remarkable capacity to adapt.
Dr. Yolanda Cruz is a general dentist. Conservative management of the arthritic TMJ is provided within the scope of general dentistry. Surgical management — when needed — is referred to an oral and maxillofacial surgeon.
Reviewed by Dr. Yolanda Cruz, DDS · Dr. Yolanda Cruz Dentistry On The Path · Toronto, ON
Types of TMJ arthritis
"Arthritis of the TMJ" is not a single diagnosis. Several distinct processes can produce arthritic changes in the joint — and each is managed slightly differently:
- Degenerative osteoarthritis (OA) of the TMJ — by far the most common pattern seen in dental practice. It develops gradually, often following long-standing disc displacement, chronic bruxism, or repetitive joint overloading. The condyle remodels, the joint space narrows, and small osteophytes may form on the condylar head.
- Inflammatory / post-traumatic arthritis — flare-up of joint inflammation following a macrotrauma (a blow to the jaw, a fall, a motor-vehicle accident) or repeated microtrauma. The synovium becomes inflamed and the joint can be acutely painful and swollen.
- Rheumatoid arthritis (RA) involvement of the TMJ — systemic autoimmune disease that can involve the TMJ in roughly half of long-standing RA patients. The pattern is bilateral, often progressive, and is co-managed with the patient's rheumatologist.
- Psoriatic, juvenile idiopathic, or other systemic arthropathies — less common but do occur. These are also co-managed with the patient's physician or rheumatologist.
- Septic (infectious) arthritis of the TMJ — rare, but a medical emergency. Sudden, severe, hot, swollen joint with fever requires urgent referral and is outside the scope of dental care.
How the joint adapts: the pseudodisc
The TMJ has a remarkable capacity to adapt. Over time, the retrodiscal tissue — the vascular, innervated pad of tissue that originally sat behind the disc, and which is pulled into the joint space when the disc displaces forward — can transform into a tough, fibrous, scar-like pad that functions much like the original articular disc. This adaptation is called a pseudodisc.
Once a pseudodisc has formed and is doing its job, the joint can open, close, and chew comfortably again — even though the original articular disc is no longer in position. Many of the patients you would expect, based on imaging, to be in chronic pain are in fact functioning well. They have successfully adapted.
The clinical implication is important: in most cases the treatment goal is not to surgically replace or restore the disc. It is to create the right conditions for natural adaptation to occur and to protect the adaptation once it has happened. For most patients, that means supporting the joint with reversible, conservative measures.
Symptoms & what to watch for
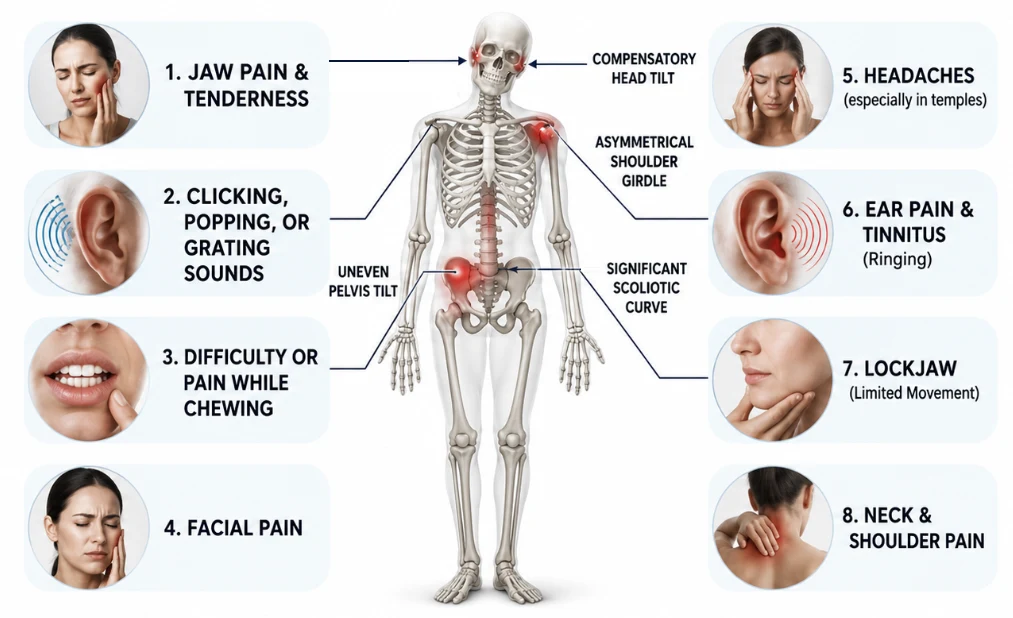
Arthritic TMJ presentations can be quiet for years and then flare. Common symptoms include:
- Deep, dull joint pain — often worse in the morning or after long periods of chewing
- Crepitus — a gritty, sand-paper-like sound or feel on opening and closing, distinct from the sharper "click" of disc displacement
- Restricted range of motion — opening less than 35–40 mm without strain
- A sense of catching or stiffness, particularly first thing in the morning
- Bite that feels uneven or different — sometimes because the condyle has shortened slightly as it remodelled
- Referred pain into the temple, ear, or behind the eye
- Flare-ups in cold weather, with stress, or with prolonged grinding/clenching
Symptoms can fluctuate. A quiet joint that suddenly becomes painful is more often a flare of the underlying arthritis or a muscular guarding response than a structural collapse — and is worth a focused evaluation rather than panic.

How an arthritic TMJ is diagnosed
Diagnosis combines clinical findings with imaging:
- Clinical exam — joint and muscle palpation, range-of-motion measurement, listening for crepitus, and assessment of bite stability
- 3D cone-beam CT (CBCT) — the imaging study that best reveals bony remodeling: osteophytes, flattening, sclerosis, erosions, and joint-space narrowing. See imaging & after your examination for what the scan involves.
- Joint Vibration Analysis (JVA) — captures the vibratory signature of the joint to help characterize the kind of pathology present; crepitus shows a different JVA pattern than disc-displacement clicking. See TMJ diagnostic technology.
- T-Scan occlusal analysis — to identify bite imbalances that may be contributing to joint loading
- Medical history — including any systemic inflammatory disease and current medications
If a systemic inflammatory or autoimmune cause is suspected, Dr. Cruz coordinates with your physician or rheumatologist before designing the dental side of the plan.
Is conservative care for an arthritic TMJ right for you?
Conservative dental management is generally appropriate when:
- Imaging shows arthritic changes (osteophytes, flattening, joint-space narrowing) but the joint is not acutely or severely destroyed
- Symptoms are intermittent, manageable, or driven by identifiable contributors (bruxism, clenching, bite imbalance, stress flares)
- The patient has not yet tried, or has only partially tried, a custom splint, bite stabilization, muscle-tension management, or home care
- The systemic component (if any) is being managed by a physician or rheumatologist
Conservative care alone may not be enough if the joint is severely destroyed, if there is a fracture, if the patient has progressive bilateral disease that is not responding to medical therapy, or if locking has become a daily structural event. In those cases Dr. Cruz refers to an oral and maxillofacial surgeon — see the note on surgery.
What the appointment feels like
Most patients describe the first arthritic-TMJ evaluation as low-key and reassuring. A typical visit involves:
- A focused conversation about your symptom history, flare pattern, sleep, stress, prior treatment, and any systemic diagnoses
- Gentle palpation of the joint capsule, masseter, temporalis, and lateral pterygoid — you'll be asked to point to anything that feels tender; the exam itself is rarely painful
- Range-of-motion measurement — open, close, side-to-side; usually painless even in arthritic joints
- Listening for crepitus with a stethoscope and (when indicated) Joint Vibration Analysis
- Review of any prior CBCT, plus a recommendation for new 3D imaging only if it is needed to characterize the bony changes
- A bite check with articulating paper and T-Scan
No injections, no drilling, no impressions on day one — the first visit is diagnostic. A written plan and cost estimate are provided before any treatment is started.
What conservative management can do
The goal is not to "cure" the arthritic joint — bony remodeling does not reverse — but to support adaptation, protect the joint, and reduce the symptom load:
Protects the joint at night
A custom oral appliance worn during sleep unloads the joint from grinding and clenching forces, which is when the heaviest damage typically occurs.
Supports natural adaptation
By stabilizing the bite and reducing joint loading, the conditions are created for retrodiscal tissue to mature into a functional pseudodisc.
Reduces flare frequency
Patients on a consistent plan — appliance, muscle management, soft-diet during flares — typically experience fewer and shorter episodes over the year.
Lowers muscle pain
Sore joints recruit the masseter and temporalis as protective splints. Reducing joint inflammation and adding Botox where indicated relieves that secondary muscle pain.
Protects the teeth
Long-standing arthritic TMD is often paired with bruxism. The appliance simultaneously protects the joint and stops accelerated wear, chipping, and cracks.
Avoids unnecessary surgery
The vast majority of arthritic TMJ presentations are managed without arthroscopy, arthrocentesis, or open joint surgery. Surgery is held in reserve for refractory cases.
Treatment options compared
Most arthritic-TMJ plans combine more than one of the categories below. The right combination depends on the diagnosis and on whether the disease is purely degenerative or part of a systemic inflammatory process.
| Option | Best for | Who provides it | Reversible? | Typical timeline |
|---|---|---|---|---|
| Conservative dental care (splint, bite stabilization, T-Scan, JVA, home program) | Most TMJ osteoarthritis and post-traumatic arthritis | Dr. Cruz (general dentistry) | Yes | Splint fitted in 2–3 visits, adjusted over 8–12 weeks; ongoing follow-up |
| Custom occlusal splint / orthotic | Bruxism, joint loading, mild–moderate arthritic TMD | Dr. Cruz | Yes | Worn nightly, adjusted as adaptation progresses |
| Botox to masseter / temporalis | Muscle hyperactivity and clenching driving joint load | Dr. Cruz | Yes — wears off in 3–4 months | Effect builds over 1–2 weeks |
| Laser therapy (Fotona / Weber / helmet) | Pain and inflammation during flares | Dr. Cruz | Yes | A short series of sessions |
| Medication management (NSAIDs, DMARDs, biologics for RA) | Inflammatory or systemic arthropathies | Physician / rheumatologist | Yes — managed by prescriber | Per medical plan |
| Arthrocentesis (joint lavage) | Refractory pain, intra-articular inflammation | Oral & maxillofacial surgeon (referral) | Minimally invasive; some lasting effect | Outpatient procedure |
| Arthroscopy | Selected refractory cases needing intra-articular visualization | Oral & maxillofacial surgeon (referral) | No | Surgical recovery |
| Open joint surgery | Reserved for severe, refractory cases | Oral & maxillofacial surgeon (referral) | No | Surgical recovery |
Dr. Cruz's clinical note
"Patients who walk in with the word arthritis in their notes are usually frightened. Someone has shown them a CBCT, pointed at the condyle, and used the word — and they've left worried that surgery is next. My first job is to put the imaging in context. A joint that looks arthritic can be a joint that has already adapted. Bone change does not equal pain."
"The treatment plan I build for an arthritic TMJ patient is unglamorous on purpose. Protect the joint at night with a custom appliance. Stabilize the bite. Calm the muscles. Get the patient out of the cycle of flare-and-clench. Re-check in three months. In most cases that's it — the joint adapts, the pseudodisc matures, and the patient stops thinking about it. The minority of cases that don't respond, I send to an oral surgeon for an arthroscopic or arthrocentesis opinion. I'm a general dentist — I know exactly where my role ends."
— Dr. Yolanda Cruz, DDS, Dr. Yolanda Cruz Dentistry On The Path, Downtown Toronto
A note on surgery & referral
Surgery for the TMJ carries real risks and should be considered a last resort. Open joint surgery in particular can interfere with the natural adaptation process described above — and is reserved for severe, refractory cases. Closed procedures such as arthrocentesis (lavage of the joint with sterile fluid) and arthroscopy (visualization and gentle treatment of the joint through small instruments) are less invasive and are sometimes used when conservative care alone is not providing enough relief.
None of these procedures are performed at this practice. Dr. Cruz refers to an experienced oral and maxillofacial surgeon when surgical assessment is appropriate, and continues to co-manage the dental and splint side of care alongside the surgical plan.
Medication management of systemic inflammatory arthropathies (rheumatoid arthritis, psoriatic arthritis, juvenile idiopathic arthritis, etc.) is led by the patient's physician or rheumatologist — not the dentist. Dr. Cruz coordinates with the medical team and provides the dental component of care.
Risks & considerations
- Bony remodeling is not reversible — conservative care supports adaptation and reduces symptoms; it does not "regrow" the condyle
- Custom appliances require an adjustment period and may temporarily change how the bite feels; the splint is adjusted at follow-up visits
- Botox to the masseter/temporalis can cause short-term bruising, mild asymmetry, or a temporarily weaker chewing feel; effects wear off in 3–4 months
- Untreated arthritic TMD can lead to accelerated tooth wear, bite collapse, and gradually progressive joint changes
- A small number of arthritic TMJ cases progress despite conservative care and may benefit from surgical assessment — referral to an oral and maxillofacial surgeon is part of the plan
- Systemic inflammatory arthritis (RA, psoriatic, JIA) requires medical management alongside any dental care
- Septic arthritis of the TMJ — sudden, severe, hot, swollen joint with fever — is a medical emergency and is not a dental scenario
Frequently asked questions about the arthritic TMJ
No — not for the majority of patients. Many people have flattening, osteophytes, and joint-space narrowing on CBCT but experience little or no symptoms because the joint has adapted: a pseudodisc has formed from the retrodiscal tissue, and the joint functions comfortably. Imaging findings alone do not predict pain or disability. The clinical picture matters more than the radiograph.
The bony changes (osteophytes, flattening, condylar remodeling) are not reversed by any current dental treatment. What conservative care does is create the right conditions for the joint to adapt — supporting pseudodisc formation, reducing inflammation, protecting against further loading, and managing flares. Most patients reach a stable, comfortable steady state even though the imaging looks unchanged.
Probably not. The vast majority of arthritic TMJ patients seen in general dentistry are managed conservatively — appliance therapy, bite stabilization, muscle management, and home care. Closed procedures like arthrocentesis or arthroscopy are reserved for cases that don't respond, and open joint surgery is rarer still. When surgical assessment is appropriate, Dr. Cruz refers you to an oral and maxillofacial surgeon. See the note on surgery.
Yes — the dental component (splint therapy, bite stabilization, muscle management, protection from grinding) is provided here. The medical component — DMARDs, biologics, systemic inflammation management — stays with your rheumatologist, and Dr. Cruz will coordinate with them. RA involvement of the TMJ is most often bilateral and progressive, and the two clinicians work together to keep the joint as comfortable and functional as possible.
Clicking is a sharper, discrete pop that typically indicates disc displacement — the disc snapping into and out of position. Crepitus is a continuous, gritty, sand-paper-like sound or feeling that suggests bony-on-bony or rough-cartilage surfaces moving against each other — an arthritic finding. Joint Vibration Analysis can characterize the difference objectively. See clicking & popping for the disc-displacement side.
Coverage varies by plan. Many Canadian extended-health and dental plans cover part of a custom occlusal appliance and some diagnostic procedures. CBCT, Botox for TMD, and laser therapy are often fee-for-service. Surgical procedures (arthrocentesis, arthroscopy) are typically billed through provincial health insurance when performed by an oral and maxillofacial surgeon in a hospital setting. We provide documentation for pre-authorization wherever possible, and the CDCP page outlines what's eligible under the federal plan.
Medical Disclaimer
This content is for informational purposes only and does not constitute dental or medical advice, diagnosis, or treatment. Arthritic conditions of the temporomandibular joint have multiple possible causes — degenerative, post-traumatic, and systemic inflammatory — and treatment outcomes vary by individual. Systemic arthropathies (rheumatoid, psoriatic, juvenile idiopathic, etc.) require management by a physician or rheumatologist. Severe, refractory, or structural cases may require referral to an oral and maxillofacial surgeon. Consult Dr. Yolanda Cruz or another qualified dental professional regarding your symptoms and treatment options. Individual results may vary.
Worried about an arthritic TMJ? Get a conservative-first evaluation in downtown Toronto.
Book a focused evaluation with Dr. Cruz. You'll leave with a clear picture of what your imaging actually shows, a working diagnosis, and a written plan — no commitment to treatment on day one.