Recapturing the Dislocated Disc — Downtown Toronto
A conservative, appliance-based protocol for early and moderate anterior disc displacement — provided within the scope of general dentistry by Dr. Yolanda Cruz at our office on the PATH at Bay & Queen.
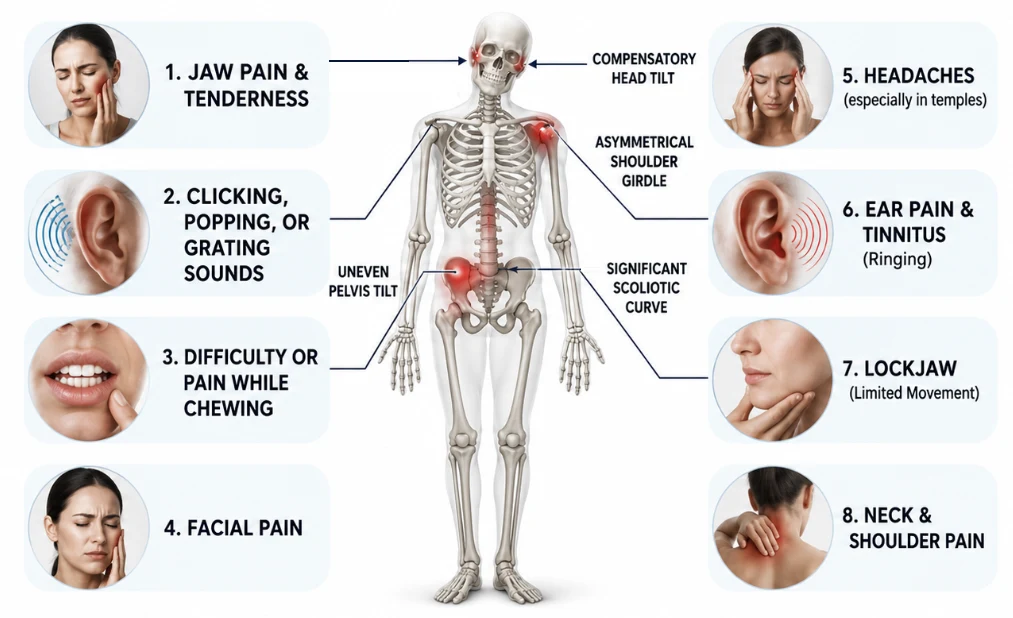
Inside each jaw joint is a small cushion of cartilage called the articular disc. It sits between the condyle of the lower jaw and the glenoid fossa of the temporal bone, acting as a shock absorber that allows smooth, comfortable opening and closing. In many people with TMD, this disc has shifted out of its proper position — a condition called anterior disc displacement or disc dislocation. When the disc is displaced, the clicking, popping, or locking sensations many TMD patients experience are often the sound of the condyle catching and sliding over the edge of the displaced disc as the mouth opens and closes. In early or moderate stages, it is sometimes possible to reposition the disc back to where it belongs using carefully fitted oral appliances. This is called disc recapturing. Schedule a consultation with Dr. Cruz or call 416-595-5490.
What disc displacement actually is
The temporomandibular joint is one of the few joints in the body that both rotates and translates — the condyle rotates against the disc, and the disc-condyle unit slides forward along the articular eminence as the mouth opens. When the posterior ligament (the retrodiscal tissue) loses its ability to pull the disc back, the disc migrates anteriorly and the condyle starts loading the retrodiscal tissue directly instead of the disc.
Two clinical pictures follow. In disc displacement with reduction, the disc is forward when the mouth is closed, but the condyle "recaptures" the disc on opening — producing the characteristic opening click. In disc displacement without reduction, the disc never reduces back onto the condyle — the patient often presents with a sudden loss of opening (the "closed lock") and the clicking actually disappears.
Dr. Yolanda Cruz is a general dentist. Disc-recapturing care is provided within the scope of general dentistry; surgical disc repositioning is referred to an oral and maxillofacial surgeon.
Reviewed by Dr. Yolanda Cruz, DDS · Dr. Yolanda Cruz Dentistry On The Path · Toronto, ON
How recapturing the disc actually works
The goal of disc recapturing is to find the jaw position at which the disc is captured by the condyle — usually by guiding the lower jaw slightly forward of its habitual resting position so the condyle sits under, rather than behind, the disc. When the jaw is held there, the click typically stops, because the condyle is no longer sliding over the displaced disc.
That position is found clinically — combining patient-reported feel, joint sounds, palpation, T-Scan occlusal analysis, and (often) Joint Vibration Analysis. Once the position is identified, a custom anterior repositioning appliance (also called an ARA or anterior repositioning splint) is fabricated to hold the mandible there during function and at rest.
The disc cannot be "snapped back" mechanically. What changes over time is the surrounding tissue: the retrodiscal ligament gradually remodels, the disc adapts, and the joint settles into a less painful, less symptomatic state. This is months of consistent positioning, not a single appointment.
MRI imaging and who is actually a candidate
Disc recapturing is not appropriate for every patient. The longer a disc has been displaced, the more it deforms — from biconcave (its healthy shape) to flattened, then folded, then perforated. A folded or perforated disc cannot be stably recaptured. An MRI of the TMJ is typically required to confirm whether the disc is recapturable before treatment begins. CBCT shows the bone but not the disc itself; MRI is the imaging modality of choice for soft-tissue staging.
You are most likely a candidate if:
- Opening produces a single reproducible click, and closing produces a softer reciprocal click
- The displacement is recent — weeks or a few months, not years
- MRI shows the disc is still biconcave or only mildly deformed
- You do not have an active closed lock at the time of evaluation
- Your bite has not yet collapsed into a position the joint can no longer accommodate
You are likely not a candidate — and would be managed differently — if:
- The click has been present for years and is now silent (suggests progression to displacement without reduction)
- MRI shows a deformed, folded, or perforated disc, or significant condylar resorption
- You currently have a closed lock — see treating the locked jaw
- The joint shows arthritic changes — see managing the arthritic TMJ
The two-appliance protocol — what it actually involves
Disc recapturing is delivered as a phased orthopedic protocol over several months. At Dr. Cruz's practice it typically combines:
- A daytime anterior repositioning appliance — thin, fitted to the lower arch, worn during waking hours to hold the mandible in the disc-capturing position during chewing and speaking
- A nighttime stabilization or repositioning appliance — protects against bruxism and maintains the position during sleep, when most clenching and grinding load occurs
- Periodic adjustments — the appliance is refined every 2–4 weeks based on symptom response, T-Scan occlusal data, and joint sounds (often re-checked with Joint Vibration Analysis)
- Adjunctive therapy when indicated — including Fotona laser therapy for the retrodiscal tissue and adjacent muscles, or Botox to the masseter / temporalis when muscular hyperactivity is loading the joint
- Imaging review — baseline MRI to stage the disc; CBCT when hard-tissue evaluation is indicated
- Home program — soft-food guidance during initial weeks, posture and jaw-rest education, and avoidance of wide opening
What treatment feels like, day by day
Most patients describe the first week as the biggest adjustment. You'll notice:
- A new "forward" feel to the bite when the appliance is in — speech may sound slightly different for the first few days
- The opening click is usually gone immediately when the appliance is seated correctly — this is often the first sign the position is right
- A few days of mild masseter or temporalis soreness as the muscles learn the new resting length
- Less ear pressure and fewer temple-pattern headaches within 1–2 weeks for many patients
- Eating takes a little planning — soft foods first, smaller bites, no wide opening for the first weeks
There are no injections on day one, no drilling, and no permanent changes to the bite during the recapture phase. Everything in the active phase is reversible by removing the appliance.
What disc recapturing can do for you
When the disc is recaptured and the joint settles, several things tend to change in concert:
The click stops — usually right away
When the appliance is seated and the disc is captured, the opening and closing click disappears. Most patients notice this on day one.
The risk of progression drops
Recapturing the disc and offloading the retrodiscal tissue reduces the risk of progressing to displacement without reduction (closed lock) and the cascade of arthritic changes that follows.
Joint pain decreases over weeks
Pre-auricular tenderness, ear pressure, and one-sided headaches often improve over 2–6 weeks as the retrodiscal tissue is no longer being loaded with every chew.
Wider, more comfortable opening
As the joint settles, opening becomes smoother and less guarded — chewing fibrous food and yawning feel safer again.
Reversible — no surgery, no irreversible bite change
The recapture phase changes nothing permanent. If it doesn't work for you, the appliance is removed and other options remain open.
Tooth-wear protection in parallel
Because a stabilizing nighttime appliance is part of the protocol, bruxism-driven enamel wear and fractures are reduced during treatment.
Disc recapture vs. surgical repositioning vs. ongoing stabilization
When a disc is displaced, there are essentially three clinical paths. The right one depends on MRI staging, symptom load, and patient goals.
| Path | Best for | Reversible? | Typical timeline |
|---|---|---|---|
| Disc recapture with anterior repositioning appliances | Early/moderate anterior disc displacement with reduction; biconcave disc on MRI; recent onset | Yes — appliance-based, no irreversible changes during phase one | Active phase 4–6 months; followed by phase-two stabilization |
| Ongoing stabilization splint without recapture | Long-standing displacement; deformed or perforated disc; low symptom load; patients declining phase two | Yes | Indefinite — managed long-term with reviews |
| Surgical disc repositioning / arthrocentesis / arthroscopy | Severe, refractory cases; failed conservative care; structural pathology on imaging | No — surgical intervention | Coordinated with oral & maxillofacial surgeon |
| "Watch and wait" with home care only | Painless clicking, no functional limit; patient preference; very recent onset to be re-assessed | Yes | Reviewed every 6–12 months |
Phase two: making the new jaw position permanent
If disc recapturing succeeds, a second phase is needed to make the recaptured position the patient's habitual bite. Without phase two, the disc will eventually displace again when the appliances are removed — because the patient's old bite still asks the condyle to sit behind the disc.
Phase two options are individualized to the patient's bite, prior dental work, and goals. They include:
- Occlusal equilibration — selective reshaping of tooth contacts using articulating paper and T-Scan data to support the new condylar position
- Orthodontic repositioning — clear aligners or braces to move teeth into the new occlusal scheme
- Restorative dental work — onlays, crowns, or full-arch restoration where teeth have been worn or shortened by years of bruxism and a collapsed bite
- Combinations — the most common phase-two plan blends a short orthodontic phase with selective restorations on the worn dentition
- Long-term retention — a thin nightguard at the new bite, indefinitely, to protect the result from grinding
The phase-two plan is presented after the disc has been stably recaptured for several months. Cost, timeline, and any restorative work are quoted at that point — not at the start of recapture.
Dr. Cruz's clinical note
"Disc recapturing is one of the most rewarding things I do — but only when I pick the right patient. The MRI matters. If the disc is biconcave and the click is recent, the chance of stable recapture is high and the patient often leaves the first appointment without their click. If the disc is folded or the patient has been clicking for ten years and is now silent, I don't try to recapture — I'd just be loading a tissue that can't carry the position. In those cases we manage with stabilization, laser, and home care instead."
"The hardest conversation isn't the recapture itself — it's phase two. Patients want to take the appliance off and be done. I'd rather tell them honestly that without phase two the disc will go forward again, than make a promise the joint can't keep. I'd much rather guide a patient through a longer, reversible plan than rush them into restorative work that has to last decades."
— Dr. Yolanda Cruz, DDS, Dr. Yolanda Cruz Dentistry On The Path, Downtown Toronto
Risks & considerations
- Disc recapturing is not appropriate for every patient — staging on MRI is required before treatment begins
- Long-standing or perforated discs cannot be reliably recaptured; in those cases other conservative options are used
- If phase-two treatment is declined or postponed, the disc will displace again when appliances are removed — recapture alone is not a permanent solution
- Anterior repositioning appliances temporarily change how the bite feels; speech may sound slightly different for the first few days
- A small number of patients experience short-term muscle soreness or temporary changes in posterior tooth contact during the active phase — both are addressed at follow-up adjustments
- Recapture treatment requires consistent appliance wear; partial or inconsistent use significantly reduces the chance of success
- Surgical disc repositioning is reserved for severe, refractory cases and is performed by an oral and maxillofacial surgeon, not within this practice
- Outcomes vary by individual; the MRI stage at presentation is the single biggest predictor of success
Frequently asked questions about disc recapture
Candidacy is decided by MRI staging plus the clinical picture. The most predictable cases are early or moderate anterior disc displacement with reduction — a clear reproducible click, recent onset, biconcave disc on MRI, no closed lock, and a bite that hasn't yet collapsed. If MRI shows a folded or perforated disc, or if the click has been silent for years, recapture is unlikely to be stable and we discuss stabilization-based management instead.
The active recapture phase is typically four to six months of consistent daytime and nighttime appliance wear, with adjustments every 2–4 weeks. Phase two — the work to make the new position permanent — varies from a single occlusal equilibration session to a longer course of clear aligners and selective restorative work. The full timeline, including phase two, is reviewed individually after the active phase is complete.
Coverage varies by plan. Many Canadian extended-health and dental plans cover part of the cost of custom occlusal appliances; MRI imaging is generally covered under OHIP when ordered for clinical indication. Phase-two restorative work and aligners are typically fee-for-service. We provide documentation for pre-authorization wherever possible. The CDCP page outlines what is eligible under the federal plan.
Yes — if phase two is skipped. Without occlusal equilibration, orthodontic repositioning, or restorative work to support the new condylar position, the patient's existing bite will pull the jaw back to its previous resting position and the disc will displace again. The whole reason phase two exists is to make the recaptured position the new habitual bite so it holds without appliances.
This is the reason the active phase is reversible. If after several weeks the disc isn't stably captured — the click persists in the appliance, or MRI shows the disc isn't sitting under the condyle — we shift to a stabilization approach, often combined with laser therapy and home care. The joint can be managed comfortably without recapture; in a small minority of refractory cases, Dr. Cruz refers to an oral and maxillofacial surgeon for surgical assessment.
The practice is at 390 Bay St., Concourse Level, Unit C006 — on the PATH at the corner of Bay & Queen, downtown Toronto. The TTC Queen station is one block away and there is underground parking nearby. Full directions and accessibility notes are on the parking & directions page.
Medical Disclaimer
This content is for informational purposes only and does not constitute dental or medical advice, diagnosis, or treatment. Disc displacement is staged by MRI and clinical examination; not every displaced disc is recapturable, and some cases require referral to an oral and maxillofacial surgeon. Disc recapturing is provided within the scope of general dentistry. Consult Dr. Yolanda Cruz or another qualified dental professional regarding your symptoms and treatment options. Individual results may vary.
Wondering whether your disc can be recaptured?
Book a focused TMJ evaluation with Dr. Cruz in downtown Toronto. You'll leave with a working diagnosis, a clear sense of whether recapture is an option, and a written plan — no commitment to treatment on day one.