Orthopedic TMJ Treatment in Downtown Toronto
A musculoskeletal approach to TMJ/TMD — protecting the joint, allowing damaged tissues to heal, and stabilizing the bite so the problem does not return. Provided by Dr. Yolanda Cruz at our office on the PATH at Bay & Queen.
TMJ disorders are fundamentally musculoskeletal conditions involving bones, joints, cartilage, and the muscles that move them. Orthopedic TMJ treatment addresses the jaw system the same way a sports medicine doctor or physiotherapist might approach a knee or shoulder injury — by understanding the underlying structural problem and using the right type of appliance or intervention to support healing and restore healthy function. Dr. Yolanda Cruz is a general dentist, and orthopedic TMJ care is provided within the scope of general dentistry. Schedule your TMJ consultation or call 416-595-5490.
Different patients need different approaches depending on the state of their joints, the condition of their bite, and how far the disorder has progressed. There is no single appliance that works for everyone — the most appropriate appliance and protocol are determined by a thorough diagnostic examination. See our TMJ treatment overview for the broader treatment context.
What orthopedic TMJ treatment is
The temporomandibular joint is a true synovial joint — with a condyle, an articular disc, ligaments, capsular tissue, and an inflammatory response when overloaded. When that joint is irritated, dislocated, arthritic, or chronically clenched against, the same orthopedic principles that apply to a knee or shoulder apply to the jaw: protect, unload, allow inflammation to settle, then stabilize.
An orthopedic TMJ approach therefore prioritizes reducing the forces on the joint before introducing anything irreversible. Most patients wear a custom appliance — an orthotic, decompression splint, or anterior repositioning appliance — that is engineered against their own bite to take the joint out of the harmful position it sits in during clenching and bruxism.
This is different from a generic boil-and-bite night guard. The appliance is designed using bite analysis, joint vibration data, and (when indicated) CBCT imaging — and is adjusted across follow-up visits as the joint responds.
Reviewed by Dr. Yolanda Cruz, DDS · Dr. Yolanda Cruz Dentistry On The Path · Toronto, ON

The general goals of orthopedic TMJ treatment
Whether the underlying picture is muscle hyperactivity, disc displacement, or early arthritic change, the same four orthopedic goals shape the plan:
- Reduce or eliminate inflammation in the jaw joint by protecting it from the forces that have been aggravating it (clenching, grinding, traumatic occlusion).
- Allow the damaged tissues within the joint to heal — the articular disc, the retrodiscal tissue, the capsule, the synovial lining.
- Stabilize the bite and the jaw position so that the same problem does not return when the appliance is removed.
- Support healthy long-term function through ongoing wear of an appropriate appliance, predominantly overnight, indefinitely for some patients.
Most patients wear their appliance primarily during sleep. Sleep is when the jaw muscles undergo their most intense activity grinding and clenching, and when the joint is most vulnerable to ongoing irritation. Protecting the joint overnight allows it to heal during the day.
A phased orthopedic approach
Orthopedic TMJ treatment is sequenced, not simultaneous. Each phase is dependent on the response of the previous one, and patients are re-evaluated at each step before moving on.
- Phase 1 — Diagnosis & baseline. Clinical exam, joint and muscle palpation, range-of-motion testing, T-Scan occlusal analysis, Joint Vibration Analysis (JVA), and CBCT imaging when hard-tissue evaluation is indicated — see diagnostic technology.
- Phase 2 — Decompression / orthotic phase. A custom appliance is fabricated against your own bite to unload the joint and break the bruxism/clenching cycle. Adjusted across 3–6 follow-up visits over 8–12 weeks.
- Phase 3 — Stabilization. Once symptoms are quiet and JVA/T-Scan readings improve, the appliance is refined to a long-term stabilization position. Most patients continue overnight wear indefinitely.
- Phase 4 — Definitive occlusal planning (if indicated). A small subset of patients with a confirmed long-standing bite collapse may be candidates for orthodontic refinement or selective occlusal equilibration — only after the joint is stable and only with informed consent.
- Phase 5 — Long-term monitoring. Periodic re-examination, T-Scan and JVA checks, and appliance maintenance.
The appliances we use orthopedically
"Orthopedic appliance" is an umbrella term. The specific device is chosen based on the diagnosis — what's loading the joint, where the disc sits, what the occlusion looks like, and whether the masticatory muscles are hypertrophied. Most patients receive one of the following:
- TMJ stabilization appliance. A full-coverage flat-plane orthotic that allows the condyles to seat into a comfortable position; the workhorse for joint pathology, bruxism, and clenching — see TMJ stabilization appliance.
- Anterior repositioning appliance (ARA). Positions the lower jaw slightly forward to recapture a displaced disc and unload the retrodiscal tissue — used for selected disc-displacement presentations.
- Decompression appliance. An orthotic with anterior contact only, designed to disengage posterior occlusion and rapidly relieve muscle hyperactivity in acute flare-ups.
- Soft-tissue conditioning appliance. A short-term transitional device used for the first few weeks of a severe muscle-pain flare before a definitive orthotic is fabricated.
- Daytime micro-appliance. A discreet partial-coverage appliance used by selected daytime clenchers when habit-reversal training alone is not enough.
For a deeper overview of every appliance type used at this practice and how they are selected, see our oral appliances page and appliance design, fit and thickness.
Where muscle hyperactivity is the dominant problem, orthopedic care is frequently combined with Botox to the masseter and temporalis and with TMJ dental laser therapy to reduce inflammation and accelerate the joint's recovery.
Is orthopedic TMJ treatment right for you?
An orthopedic approach is generally appropriate if you experience any of the following — particularly when conservative single-modality care (a generic night guard, occasional anti-inflammatories) has not held:
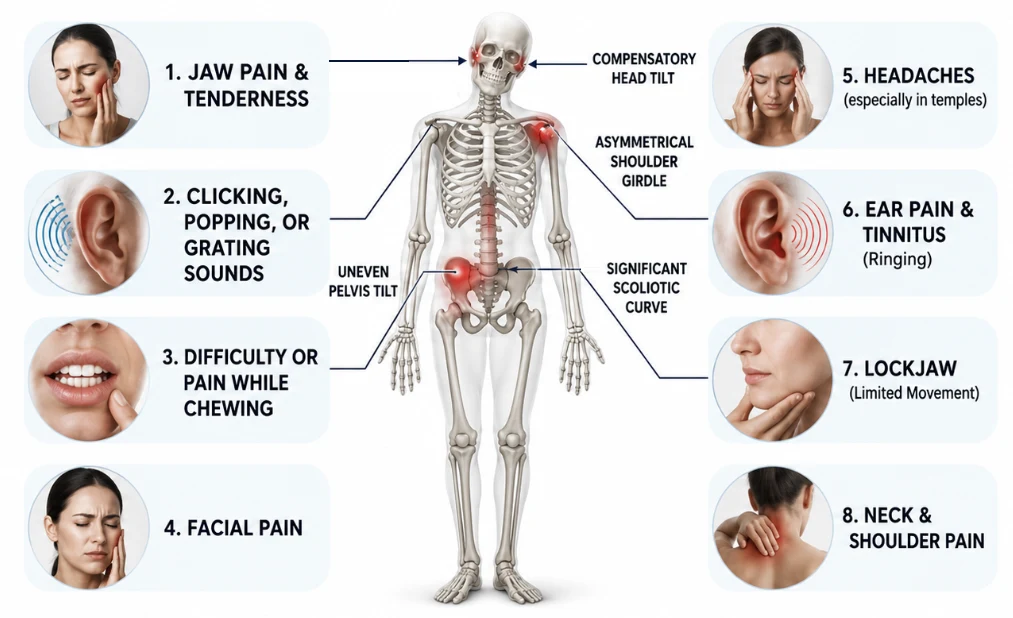
- Persistent or recurrent jaw pain, especially with chewing, wide opening, or after sleep
- Clicking, popping, or grating sounds that have been increasing in frequency or have started to be accompanied by discomfort
- A history of jaw catching, deviating, or briefly locking — open or closed
- Bruxism (teeth grinding) with visible wear facets, tooth chipping, or sensitivity
- A bite that feels uneven, shifted, or different than it used to
- Tension-pattern headaches in the temples or at the base of the skull that worsen on grinding nights
- An over-the-counter night guard that hasn't helped — or has made symptoms worse
- A previously diagnosed TMJ disorder where symptoms have returned
An orthopedic plan at this practice may not be the right starting point if your symptoms are acute and trauma-related (e.g., a recent fracture or dislocation), or if imaging suggests advanced structural pathology in the joint itself that needs surgical assessment first. In those cases Dr. Cruz will refer you to an oral and maxillofacial surgeon before any orthopedic appliance is considered.
What the orthopedic appointment feels like
Most patients tell us the anticipation is worse than the visit itself. A first orthopedic TMJ evaluation involves:
- A focused conversation about your symptoms, history, sleep, stress, and any prior treatment — including any appliances or splints you've worn before
- Gentle palpation of the masseter, temporalis, and lateral pterygoid muscles, and the joint capsule itself — you'll be asked to point out anything tender
- A range-of-motion assessment (open, close, side-to-side, protrusive) — usually painless
- A bite check with articulating paper, T-Scan occlusal analysis, and (when indicated) Joint Vibration Analysis to characterize the joint sounds
- Review of any prior imaging, plus a recommendation for 3D CBCT only if hard-tissue evaluation is needed — see imaging & after your examination
No appliance impressions on day one — the first visit is diagnostic. A written plan and cost estimate follow before any orthopedic appliance is fabricated.
What an orthopedic plan can do for you
An orthopedic TMJ plan is designed to address contributing factors at the joint level, not just to mask symptoms.
Protects the joint from harmful load
A custom appliance unloads the condyle and disc — the same orthopedic principle behind a brace, sling, or unloader used for a knee or shoulder.
Lets inflamed tissue heal
Reducing intra-articular load gives the disc, capsule, and retrodiscal tissue a chance to settle — often the first time in years.
Quieter joint, easier function
As inflammation settles, opening, chewing, and speaking become less guarded — and clicking often quiets, even if it doesn't fully resolve.
Stabilizes the bite
The appliance is fine-tuned across follow-ups using T-Scan data so that the jaw settles into a position the joint can tolerate long term.
Protects your teeth
Bruxism and joint dysfunction cause accelerated wear, cracked cusps, and bite collapse. Orthopedic appliance wear limits that long-term damage.
Reversible, sequenced, conservative
Nothing irreversible happens early. The appliance can be removed, refined, or replaced — and no orthodontics or equilibration is undertaken until the joint is quiet.
Orthopedic appliance vs. generic splint vs. Botox
Patients often arrive having already tried one of the options below. The table is a general orientation — the right combination depends on the diagnosis.
| Option | Best for | Addresses joint mechanics? | Reversible? | Typical timeline |
|---|---|---|---|---|
| Orthopedic TMJ appliance (stabilization / ARA / decompression) | Disc displacement, joint pathology, mild–moderate arthritis, refractory bruxism | Yes — designed to unload, reposition, and stabilize | Yes | Fitted in 2–3 visits; adjusted over 8–12 weeks; long-term overnight wear |
| Generic over-the-counter night guard | Mild bruxism, no joint involvement | No — bulk only, no occlusal control | Yes | Same day — but can worsen TMD in some patients |
| Custom flat-plane night guard (no orthopedic positioning) | Tooth protection in stable joints | Partial — protects teeth, does not actively reposition | Yes | 2 visits, no follow-up adjustments |
| Botox to masseter / temporalis | Muscle-dominant TMD, hypertrophy, clenching | Indirectly — reduces muscle load on the joint | Yes — wears off in 3–4 months | Effect builds over 1–2 weeks |
| Surgical referral (arthroscopy / arthrocentesis / open surgery) | Severe, refractory, structural cases | Yes — directly | No | Coordinated with an oral and maxillofacial surgeon |
Dr. Cruz's clinical note on the orthopedic approach
"I think the most useful frame I can give a new TMJ patient is the orthopedic one. If you tore the meniscus in your knee, you wouldn't ask for a stronger painkiller — you'd ask what's loading that joint, and how do we take the load off so it can heal? The jaw deserves the same logic."
"That's why I rarely start with anything irreversible. The first orthopedic appliance is reversible. The way I adjust it is reversible. The Botox we sometimes add is reversible. We earn the right to talk about anything permanent — orthodontic refinement, occlusal equilibration, restorative work — only after the joint is quiet and we know the position is stable. For most of my patients, we never need to get to that stage."
"I'm a general dentist, not an oral surgeon. The vast majority of TMJ/TMD I see can be managed with an orthopedic plan, without surgery — but I'll always tell you when it's time to consult one."
— Dr. Yolanda Cruz, DDS, Dr. Yolanda Cruz Dentistry On The Path, Downtown Toronto
Risks & considerations
- Orthopedic appliances require an adjustment period — the bite can feel different for the first 1–2 weeks
- Some patients experience temporary tooth tenderness, salivation changes, or a feeling of the bite shifting as the joint repositions
- Long-term overnight wear is often required — orthopedic appliances are usually not a short course of treatment
- A small minority of patients develop a "bite change" once the joint stabilizes, which may require selective occlusal refinement or orthodontic input
- Generic boil-and-bite or drugstore night guards can worsen some orthopedic presentations — they should not be used as a substitute
- Severe disc derangement, advanced arthritis, ankylosis, or trauma may require referral to an oral and maxillofacial surgeon before any appliance is fabricated
- Chronic TMJ/TMD may need long-term management rather than a one-time cure
Frequently asked questions about orthopedic TMJ treatment
Orthopedic TMJ treatment uses a custom appliance designed to unload, reposition, and stabilize the temporomandibular joint — not just to cover the teeth. A regular over-the-counter night guard adds bulk between the teeth but does not control occlusal contacts, condylar position, or muscle loading. An orthopedic appliance is engineered against your own bite using T-Scan, articulating paper, and (when indicated) Joint Vibration Analysis — and is adjusted across multiple follow-up visits as the joint responds. It applies the same orthopedic principles used for any other inflamed synovial joint in the body: protect, unload, allow healing, then stabilize.
The active orthopedic phase — when the appliance is being adjusted as the joint settles — usually takes 8–12 weeks. After that, most patients continue overnight wear as a long-term stabilization measure, often indefinitely, much like wearing an orthotic insole for a chronic foot or knee issue. The appliance is checked and refined at periodic recall visits.
The appliance itself is reversible — it can be removed, refined, or replaced. Once the joint is unloaded, some patients do experience a "bite change" because the condyles can finally settle into a less stressed position; this is usually a sign that the previous bite was actually compensating for joint dysfunction. If a refined bite is desired after the joint is stable, options include selective occlusal adjustment, orthodontic refinement, or definitive restorative work — all undertaken only with informed consent, and only after the orthopedic phase has succeeded.
Yes — combining modalities is often more effective than any single intervention. Botox to the masseter and temporalis reduces muscle load on the joint while the orthopedic appliance does its work. Fotona and Weber laser therapy can accelerate the settling of inflammation. Combination care is matched to the diagnosis; not every patient needs all three.
Coverage varies by plan. Many Canadian extended-health and dental plans cover part of a custom occlusal appliance and some diagnostic procedures (T-Scan, JVA, CBCT). Botox for TMD and laser therapy are usually fee-for-service. We provide documentation for pre-authorization wherever possible. The CDCP page outlines what's eligible under the federal plan.
A custom night guard from a general dental visit is usually a flat-plane tooth-protection appliance. It may protect teeth from grinding wear but does not actively reposition the condyles or stabilize the bite. An orthopedic TMJ appliance is designed against bite analysis (T-Scan), joint sound data (JVA), and condyle position — and is adjusted across multiple visits, not delivered once and forgotten. If a previous splint hasn't worked, that doesn't mean splints don't work; it usually means the splint wasn't designed orthopedically.
Medical Disclaimer
This content is for informational purposes only and does not constitute dental or medical advice, diagnosis, or treatment. TMJ/TMD disorders have multiple possible causes and treatment outcomes vary by individual. Some cases require referral to an oral and maxillofacial surgeon or another specialist before any orthopedic appliance is fabricated. Consult Dr. Yolanda Cruz or another qualified dental professional regarding your symptoms and treatment options. Individual results may vary.
Ready for an orthopedic TMJ consultation in downtown Toronto?
Book a focused TMJ/TMD evaluation with Dr. Cruz. You'll leave with a working diagnosis and a written plan — no commitment to treatment on day one.