Sleep Apnea Treatment in Downtown Toronto
Dental sleep medicine for snoring and obstructive sleep apnea — custom oral appliance therapy, Fotona NightLase® laser, and collaboration with sleep physicians. Provided by Dr. Yolanda Cruz at our office on the PATH at Bay & Queen.
Sleep apnea is a medical condition. A formal diagnosis can only be made by a physician following a sleep study. Dr. Cruz works in collaboration with sleep physicians and can facilitate referrals when indicated. Her role is in the dental assessment and management of sleep-disordered breathing — specifically oral appliance therapy and laser-based treatments. Schedule a sleep apnea consultation or call 416-595-5490.
Dr. Yolanda Cruz is a general dentist. The following services are provided within the scope of general dentistry.

A dental role within a medical condition
Obstructive sleep apnea (OSA) is diagnosed by sleep physicians on the basis of a sleep study (polysomnography or a validated home sleep apnea test) that measures the Apnea–Hypopnea Index (AHI). Dr. Cruz's practice does not diagnose OSA — but once a diagnosis is in hand, dental sleep medicine can play a defined role.
That role is the fabrication and management of custom oral appliances (mandibular advancement devices), Fotona NightLase® laser therapy for snoring and mild airway issues, and ongoing collaboration with the patient's referring sleep physician. When findings suggest CPAP, ENT involvement, or surgical referral are more appropriate, Dr. Cruz will refer.
Dr. Yolanda Cruz is a general dentist. All services described on this page are provided within the scope of general dentistry.
Reviewed by Dr. Yolanda Cruz, DDS · Dr. Yolanda Cruz Dentistry On The Path · Toronto, ON
Treatment options for obstructive sleep apnea
Treatment is selected against the diagnosed severity, the patient's tolerance of CPAP, and any airway, dental, or TMJ findings. The dental options (oral appliance therapy and NightLase®) are provided directly at this practice; the others are managed in collaboration with sleep physicians, ENT surgeons, and maxillofacial surgeons.
CPAP (Continuous Positive Airway Pressure)
The most widely prescribed treatment for moderate-to-severe OSA. A CPAP machine delivers a continuous stream of pressurized air through a mask worn during sleep to maintain airway patency. Compliance rates vary, and some patients find long-term use difficult.
Oral Appliance Therapy (Mandibular Advancement Device)
Custom-fitted dental appliances that position the lower jaw slightly forward during sleep, widening the pharyngeal airway. Per AASM and AADSM guidelines, oral appliances are a recommended option for mild-to-moderate OSA, and an alternative for severe OSA in patients unable to tolerate CPAP.
Fotona NightLase® Laser Therapy
A non-invasive, in-office laser treatment that applies photothermal energy to the soft palate and surrounding throat tissues, producing a firming effect that may reduce airway collapse and snoring. Delivered over a series of three appointments, with no needles, no anesthesia, and no recovery period.
Lifestyle Modifications
Weight management, positional therapy (sleeping on the side), reducing alcohol before bed, and treating nasal congestion are commonly recommended in conjunction with other treatments.
Surgical Options
Procedures such as tonsillectomy and adenoidectomy (particularly in children), uvulopalatopharyngoplasty (UPPP), and orthognathic surgery are managed by ENT and maxillofacial surgeons. Dr. Cruz will refer to the appropriate surgical specialist when indicated.
Adjunctive Aids
Nasal-dilator devices such as Mute nose cones may improve nasal breathing in patients whose airway issues are partially driven by nasal congestion. These are an adjunct, not a stand-alone OSA treatment.
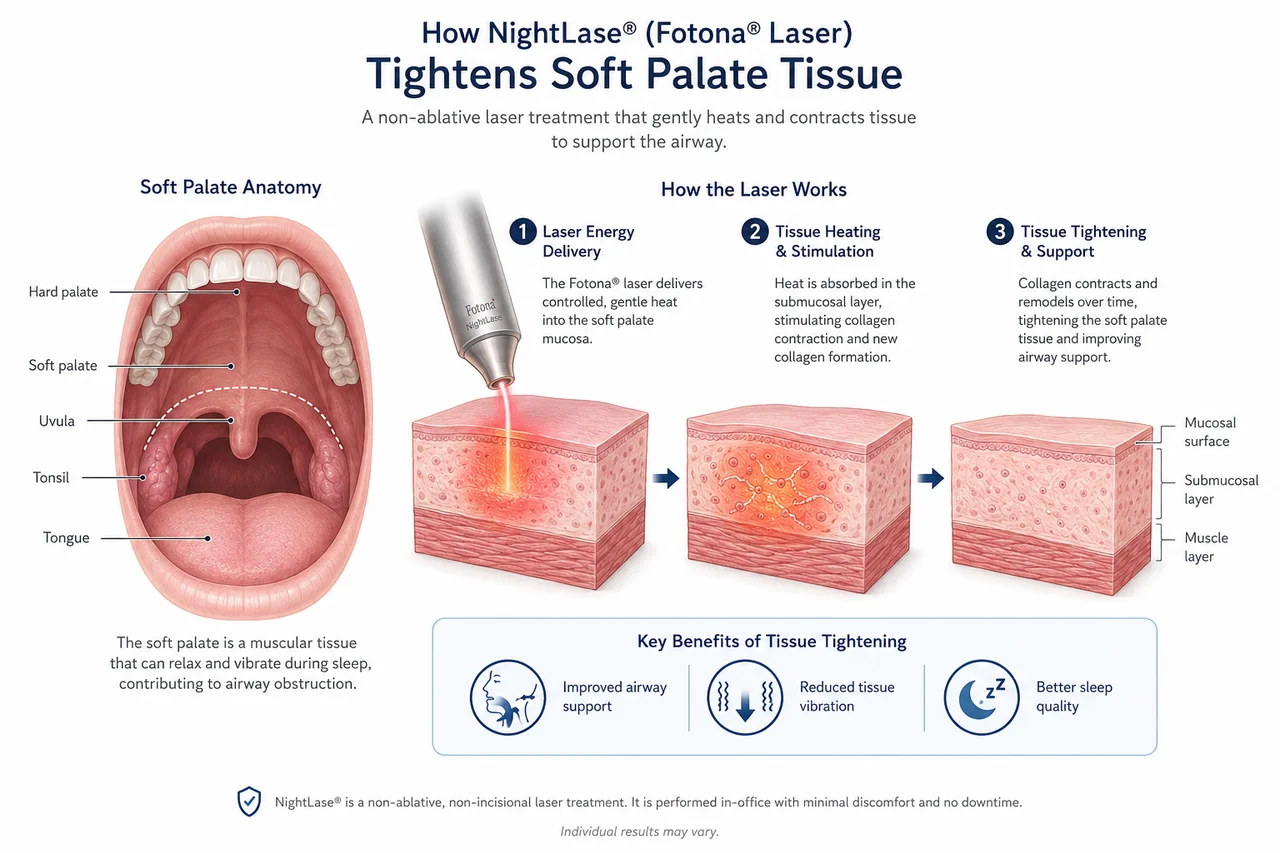
Understanding the Science Behind NightLase®
NightLase® targets the soft tissues at the back of the throat using controlled laser energy. The treatment is designed to promote tissue tightening and support the airway, which may help reduce the tissue vibration associated with snoring. This diagram is provided for educational purposes to illustrate the treatment process and anatomy involved.
Treatment by severity
Severity of obstructive sleep apnea is graded by the Apnea–Hypopnea Index (AHI) — the average number of apnea and hypopnea events per hour of sleep, as scored on a diagnostic sleep study by a sleep physician. The American Academy of Sleep Medicine (AASM) and the American Academy of Dental Sleep Medicine (AADSM) publish guidance on which treatments are appropriate at each severity level.
| Severity | AHI (events / hour) | Treatment options |
|---|---|---|
| Mild OSA | 5 – 15 | Oral appliance (recommended option) |
| Moderate OSA | 15 – 30 | CPAP or oral appliance |
| Severe OSA | 30+ | CPAP; oral appliance for CPAP-intolerant patients |
Source: American Academy of Sleep Medicine (AASM) and American Academy of Dental Sleep Medicine (AADSM) clinical practice guidelines. The treatment selected for any individual is based on the sleep physician's recommendation and the patient's own clinical picture.
Is a dental sleep apnea evaluation right for you?
A dental consultation about sleep apnea or snoring is generally appropriate if any of the following applies — particularly when a sleep study has already been done or is being arranged:
- You have been diagnosed with mild or moderate OSA and want to consider an oral appliance instead of, or alongside, CPAP
- You have severe OSA and have not been able to tolerate CPAP
- A bed partner reports loud, regular snoring or witnessed pauses in your breathing during sleep
- You experience excessive daytime sleepiness, morning headaches, or unrefreshing sleep
- You wake with a dry mouth, sore throat, or feel as though you have been "fighting for air" overnight
- You also have TMJ/TMD symptoms — jaw pain, clicking, or bruxism — which can influence appliance design
- You have not had a sleep study but suspect airway-related sleep concerns and want to know which next step is appropriate
Dental sleep medicine at this practice may not be the right starting point if you do not yet have a sleep study and your symptoms suggest severe OSA, central sleep apnea, or an upper-airway problem better evaluated by ENT. In those cases Dr. Cruz will direct you back to a sleep physician or to ENT before any appliance is fabricated.
What the appointment feels like
The first dental sleep medicine appointment is diagnostic, not active treatment. Expect:
- A focused conversation about your sleep, snoring, witnessed apneas, daytime sleepiness, and any previous sleep study results (please bring them)
- A short questionnaire similar to the STOP-BANG tool to estimate OSA risk
- An intraoral and airway examination — tongue scalloping, tonsil grade, Mallampati position, palate shape, range of jaw protrusion
- A bite check with articulating paper and (when indicated) T-Scan occlusal analysis to identify factors that could influence appliance design
- Discussion of whether you need a sleep study, a referral to a sleep physician, or whether you already have everything needed to proceed
No appliance impressions on day one. Appliance fabrication happens only after diagnosis is in hand and a written plan and cost estimate have been provided.
What an oral appliance can do for you
For appropriately selected patients, a custom mandibular advancement device is designed to address the contributing factors and reduce the symptom load:
Quieter, more restful sleep
Forward positioning of the mandible widens the pharyngeal airway, reducing the soft-tissue vibration that produces snoring and the airway collapse that produces apneic events.
An alternative when CPAP isn't tolerated
For patients with severe OSA who cannot adapt to CPAP, an oral appliance is a guideline-recognized alternative — not a perfect substitute, but a real option.
Portable and travel-friendly
A custom appliance fits in a small case, needs no power supply, and travels easily — one of the most commonly cited reasons patients prefer it over CPAP.
Improved daytime function
When sleep-disordered breathing is being treated effectively, daytime sleepiness, concentration, and morning headache often improve over the first weeks of consistent use.
Customized & titratable
The appliance is adjustable in small increments over follow-up visits to find the position that maximizes airway opening with the minimum jaw protrusion needed.
Coordinates with TMJ care
If you also have TMJ/TMD or bruxism, appliance design can be integrated with TMJ management so that the same device does not aggravate the joint.
CPAP vs. oral appliance — how they compare
CPAP and oral appliance therapy are not in competition — each has clear indications. The table below is a general orientation. The right choice for any patient depends on the sleep study, the severity, and tolerance.
| CPAP | Oral Appliance (MAD) | |
|---|---|---|
| Best for | Moderate-to-severe OSA | Mild-to-moderate OSA; severe OSA in CPAP-intolerant patients |
| How it works | Pressurized air via mask keeps the airway open | Forward mandibular position widens the pharyngeal airway |
| Prescribed by | Sleep physician | Sleep physician + dentist (fabricated & titrated by dentist) |
| Reversible? | Yes (no permanent change) | Yes — though small bite changes are possible over years of use |
| Typical timeline | Titrated by physician; nightly use indefinitely | Fitted in 2–3 visits, titrated over 8–12 weeks, nightly use indefinitely |
| Travel / portability | Machine + power required | Small case, no power required |
| Compliance | Variable; some patients find long-term use difficult | Generally higher self-reported adherence |
What patients usually want to know
"Do I need a sleep study first?"
Yes. Obstructive sleep apnea is a medical diagnosis and oral appliance therapy is a medical treatment. A dental appliance should not be fabricated for OSA without a documented sleep study and a physician's diagnosis. If you do not yet have one, Dr. Cruz can facilitate a referral to a sleep physician.
"How much does treatment cost?"
Cost varies with the type of appliance, the number of titration visits, and whether NightLase® sessions are included. A written plan and personalized estimate are provided after the diagnostic visit. Many Canadian extended-health plans cover part of a custom oral appliance prescribed for OSA — we will help you submit. Schedule a consultation for a personalized estimate.
"I just snore — is that the same thing?"
Not necessarily. Some snoring is "simple snoring" with no apneic events; some snoring is the most obvious symptom of OSA. A sleep study is the only way to know. Read "What is sleep apnea?" and sleep tips for snoring & sleep apnea as a starting point.
"I bought a boil-and-bite snore guard online — is that the same?"
No. Generic over-the-counter snore guards are not titratable, are not designed against your bite, and are not appropriate for treating diagnosed OSA. A custom appliance is designed from intraoral scans or impressions and adjusted in small increments over follow-up visits.
Dr. Cruz's clinical note
"The most common reason patients come to me for sleep apnea is that CPAP didn't work for them — they've tried it, they couldn't tolerate the mask, and they want to know whether there's another option. The honest answer is: sometimes. An oral appliance is a real, guideline-supported alternative for mild-to-moderate OSA, and for severe OSA in patients who genuinely can't tolerate CPAP. But it is not a replacement for a sleep study and it is not a substitute for a sleep physician. I won't fabricate an appliance for somebody who doesn't have a diagnosis."
"What I will do is examine the airway, the bite, the joint, and the soft tissue, talk you through what the sleep study showed, and tell you honestly whether a dental appliance is likely to help you. If it is, we make a custom device, titrate it over a few visits, and stay in contact with your sleep physician. If it isn't, I'll tell you that too."
— Dr. Yolanda Cruz, DDS, Dr. Yolanda Cruz Dentistry On The Path, Downtown Toronto
A note on surgery
Surgical management of OSA — tonsillectomy and adenoidectomy (particularly in children), uvulopalatopharyngoplasty (UPPP), maxillomandibular advancement, hypoglossal nerve stimulation — is performed by ENT and oral & maxillofacial surgeons, not by a general dentist. These procedures are typically considered after non-surgical options have been tried or in patients with clear anatomical contributors. Dr. Cruz will refer to the appropriate surgical specialist when clinically indicated. See treating sleep apnea with oral surgery for background on what the surgical pathway involves.
Risks & considerations
- Oral appliance therapy requires an adjustment period; some patients report jaw soreness, dry mouth, or increased salivation in the first few weeks
- Long-term mandibular advancement can produce small bite changes over years of nightly use — monitored at follow-up visits
- Active TMJ/TMD, advanced periodontal disease, severely worn dentition, or insufficient teeth can affect candidacy for a MAD — design needs to account for it
- An oral appliance is not appropriate for severe OSA as a first-line treatment when CPAP is tolerated — it is an alternative, not an equal substitute
- Untreated obstructive sleep apnea is associated with hypertension, cardiovascular disease, type 2 diabetes, daytime sleepiness, and motor-vehicle accident risk
- Self-treatment with an over-the-counter snore guard, without a sleep study or dental supervision, can mask OSA symptoms without treating the underlying airway problem
- NightLase® laser therapy is non-invasive but is not a stand-alone treatment for diagnosed moderate-to-severe OSA — expectations should be set against the AHI
Frequently asked questions about sleep apnea treatment
A dentist can manage certain treatments for sleep apnea — but cannot diagnose it. Obstructive sleep apnea is diagnosed by a sleep physician on the basis of a sleep study (AHI). Once that diagnosis is in hand, a dentist trained in dental sleep medicine can fabricate a custom oral appliance (mandibular advancement device), provide Fotona NightLase® laser therapy, and coordinate care with the sleep physician. At Dr. Cruz's practice in downtown Toronto, that is the dental scope — CPAP, ENT surgery, and other medical treatments are managed elsewhere and referred when appropriate.
Coverage varies by plan. Many Canadian extended-health and dental plans cover part of a custom oral appliance prescribed for diagnosed obstructive sleep apnea. The diagnosis (sleep study report) and a physician's prescription are usually required for reimbursement. We provide documentation for pre-authorization wherever possible. The CDCP page outlines what is eligible under the federal plan.
Many patients notice quieter sleep and less morning grogginess within the first 1–2 weeks of consistent appliance use. Full titration — finding the position that maximizes airway opening with the smallest jaw advancement needed — usually takes 8–12 weeks of follow-up adjustments. A repeat sleep study is sometimes recommended after titration to confirm the appliance is reducing the AHI as intended.
Often yes — but the appliance design needs to take TMJ/TMD into account. Mandibular advancement loads the joint, so an appliance that helps the airway can aggravate the joint if not designed carefully. Dr. Cruz coordinates appliance design with TMJ treatment when both conditions are present. In some cases TMJ symptoms are managed first before an MAD is fabricated.
No. Fotona NightLase® is a non-invasive in-office laser treatment that applies photothermal energy to the soft palate to produce a firming effect. It is most useful for snoring and may help in selected mild airway cases. It is not a stand-alone treatment for diagnosed moderate-to-severe OSA and should not be presented as one. Treatment expectations are set against the diagnosed AHI.
The practice is at 390 Bay St., Concourse Level, Unit C006 — on the PATH at the corner of Bay & Queen, downtown Toronto. The TTC Queen station is one block away and there's underground parking nearby. Full directions and accessibility notes are on the parking & directions page.
Medical Disclaimer
This content is for informational purposes only and does not constitute dental or medical advice, diagnosis, or treatment. Obstructive sleep apnea is a medical condition that requires diagnosis by a sleep physician on the basis of a sleep study. Treatment outcomes vary by individual and depend on diagnosis, severity, anatomy, and adherence. Some patients require referral to a sleep physician, ENT, or maxillofacial surgeon. Consult Dr. Yolanda Cruz or another qualified dental professional regarding your symptoms and treatment options. Individual results may vary.
Ready for a sleep apnea consultation in downtown Toronto?
Book a focused dental sleep medicine evaluation with Dr. Cruz. Bring any prior sleep study results. You'll leave with a written plan, a referral pathway if you need one, and no commitment to treatment on day one.