Palate Expansion in Downtown Toronto
Non-surgical widening of the upper jaw to open the airway, make room for the tongue, and support TMJ and sleep-disordered breathing care — with Dr. Yolanda Cruz on the PATH at Bay & Queen.
Many adults and adolescents have an upper jaw (palate) that is narrower than it should be. A narrow palate means a narrower nasal airway, less room for the tongue to rest against the roof of the mouth, and crowded teeth — and all three are directly relevant to TMJ/TMD and sleep-disordered breathing. Palate expansion is a non-surgical, removable-appliance treatment that gradually widens the upper jaw over several months. Schedule a consultation or call 416-595-5490.
A narrow palate is more than a dental problem
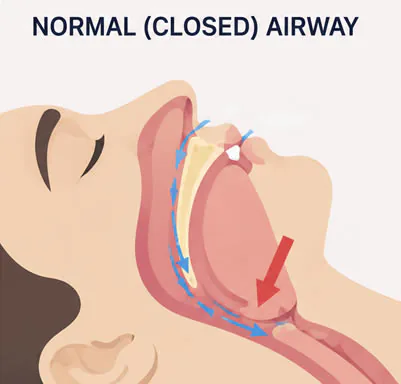
The roof of your mouth is the floor of your nose. When the upper jaw is narrow, the nasal airway is narrow too — a setup that promotes mouth breathing, snoring, and obstructive sleep apnea. A narrow arch also leaves the tongue without enough room to rest against the palate, so it falls backward and pulls the lower jaw with it, further compromising the airway.
Modern softer diets, prolonged thumb-sucking, chronic mouth breathing, and large tonsils or adenoids in childhood are all factors that can interrupt the normal lateral growth of the maxilla. The result is a maxillary transverse deficiency — and often a posterior crossbite, dental crowding, and a high-vaulted palate.
Dr. Yolanda Cruz is a general dentist. Palate expansion at this practice is provided within the scope of general dentistry, in coordination with sleep medicine and orthodontic specialists where indicated.
Reviewed by Dr. Yolanda Cruz, DDS · Dr. Yolanda Cruz Dentistry On The Path · Toronto, ON

Light, steady force — over months, not days
A custom-fabricated expansion appliance is worn in the mouth most of the time — ideally throughout the day, not just at night. The appliance carries a small expansion mechanism that is activated incrementally on a defined schedule, applying gentle lateral force across the palate.
The two halves of the upper jaw meet at the midpalatal suture. In growing children and adolescents, that suture is still patent and responds to expansion forces with true skeletal widening — this is rapid palatal expansion (RPE). In adults the suture has fused, so expansion has to either be slower and more dentoalveolar in nature, or use a bone-borne MARPE/MSE appliance that applies force directly to the skeleton rather than the teeth.
Activation is gradual on purpose. Light, steady force gives the bone, the periodontal ligament, and the surrounding soft tissues time to remodel without overload. Expansion typically continues over a period of several months, followed by an equally important retention phase.
Adults vs. children — the process is different
The most important variable in palate expansion is whether the midpalatal suture is still open. That determines which appliance design is appropriate and how the force is applied.
- Children and early adolescents — the midpalatal suture is patent. A rapid palatal expander (RPE) attached to the upper molars produces true skeletal expansion in 2–6 weeks, followed by months of retention
- Late adolescents and young adults — the suture is partially fused. Slow palatal expansion over several months can still produce a combination of skeletal and dentoalveolar widening
- Adults — the midpalatal suture is closed. Conventional tooth-borne expanders mostly tip the teeth outward rather than widen bone. A bone-borne MARPE (mini-implant-assisted rapid palatal expander) or MSE (maxillary skeletal expander) uses temporary anchorage devices in the palatal bone to apply force directly to the skeleton, enabling genuine skeletal expansion in many adult patients without surgery
- Severe adult cases — surgically-assisted rapid palatal expansion (SARPE) is performed by an oral and maxillofacial surgeon and is considered when the suture cannot be opened by MARPE/MSE alone. This is referral territory
What palate expansion can address
The following goals are the reasons palate expansion is recommended at this practice, individually or in combination:
- Widening the nasal airway, which may reduce mouth breathing and improve nasal patency
- Creating more space for the tongue to rest in the proper position against the roof of the mouth — a posture that supports a more forward mandibular position and a more open posterior airway
- Providing additional arch length for crowded teeth, reducing the need for extractions in subsequent orthodontic treatment
- Correcting a posterior crossbite, where the upper teeth sit inside the lower teeth on one or both sides
- Supporting a more forward jaw position, which is relevant to both TMD and sleep-disordered breathing
- Improving the foundation for subsequent orthodontic alignment, oral appliance therapy for sleep apnea, or TMJ orthotic work
Is palate expansion right for you?
Expansion is generally worth evaluating if you or your child experience any of the following:
- A high-vaulted, narrow upper palate visible when you open your mouth
- A posterior crossbite — upper teeth sitting inside the lower teeth on one or both sides
- Chronic mouth breathing, snoring, or a diagnosed mild-to-moderate obstructive sleep apnea
- Crowded teeth, particularly in the upper arch, with a constricted dental arch shape
- A history of chronic enlarged tonsils, adenoids, or allergies that limited nasal breathing in childhood
- A child or adolescent before their growth spurt is complete — the suture is still patent and expansion is most predictable
- An adult with a transverse maxillary deficiency who wants to explore a non-surgical option before considering SARPE
Palate expansion at this practice may not be the right starting point if your symptoms are dominated by acute joint pathology that needs to be settled first, if you have a severe skeletal discrepancy that requires orthognathic surgical planning, or if you are a child whose growth is best directed by a pediatric orthodontist. In those cases Dr. Cruz will refer you appropriately.
What the appointment feels like
Most patients find the process easier than they expect — especially after the first week. A typical course looks like this:
- A focused conversation about symptoms, airway, sleep, prior orthodontic history, and goals
- A clinical exam of the palate, arch form, occlusion, and tongue posture — plus a look at how you breathe at rest
- A 3D cone beam CT (CBCT) scan when indicated, to evaluate the midpalatal suture and the nasal airway in three dimensions
- An intraoral scan or impressions to fabricate the custom appliance
- Fitting the appliance — you will feel pressure, but not pain. The first few days involve a sense of fullness and slightly altered speech that settles quickly
- Activation on a schedule — a small key turn (RPE) or screw advance (MARPE/MSE) at defined intervals. Each activation produces a brief sensation of pressure across the nose and cheekbones that fades within minutes
No injections, no drilling, no irreversible step at the diagnostic visit. A written plan and cost estimate follow before any appliance is fabricated.
What expansion can do for you
Targeted palate expansion is designed to widen the maxilla, open the airway, and create the architectural foundation for downstream treatment:
Wider maxillary arch
The upper jaw is widened by 5–10 mm in many cases, correcting posterior crossbite and producing a broader, more natural arch form.
Improved nasal breathing
Because the palate is the floor of the nose, lateral expansion enlarges the nasal cavity — many patients report easier nasal breathing within weeks.
Better tongue posture
A broader palate gives the tongue room to rest against the roof of the mouth, which supports a more forward mandibular position and a more open posterior airway.
Adjunct to TMJ & sleep care
Expansion is often the first step before an oral appliance for sleep apnea or a TMJ orthotic, because it changes the airway and jaw posture that downstream appliances rely on.
Reduced crowding
More transverse arch length often means fewer extractions in subsequent orthodontic treatment, especially in adolescents.
Non-surgical option for adults
MARPE/MSE protocols using temporary anchorage devices give many adults a genuine skeletal expansion result without the cost or recovery of SARPE surgery.
Expansion options compared
The right expansion protocol depends on skeletal maturity, the degree of transverse deficiency, and the broader treatment plan. The table is a general orientation — the right option is determined by clinical exam and CBCT findings.
| Option | Best for | Skeletal vs. dental | Typical timeline |
|---|---|---|---|
| Rapid palatal expansion (RPE) | Children & early adolescents with patent midpalatal suture | Mostly skeletal | 2–6 weeks of active expansion + 4–6 months retention |
| Slow palatal expansion | Late adolescents & young adults with partially fused suture | Mixed skeletal + dentoalveolar | 3–6 months of active expansion + retention |
| MARPE / MSE (mini-implant-assisted) | Adults with fused suture wanting non-surgical skeletal expansion | Genuinely skeletal in many cases | 4–12 weeks active + 6+ months retention |
| Tooth-borne adult expander | Adults with mild crossbite where dentoalveolar tipping is acceptable | Mostly dentoalveolar tipping | 3–6 months of active expansion |
| SARPE (surgical referral) | Adults whose suture cannot be opened by MARPE/MSE alone | Skeletal — suture is surgically released | Coordinated with oral & maxillofacial surgeon |
After expansion — what happens next
Once the desired width is achieved, the expansion phase is over — but the treatment is not. The widened position must be retained while bone fills in across the suture and the surrounding tissues stabilize. Skipping retention is the single most common reason for relapse.
- Retention — the appliance is locked and worn passively for several months while new bone forms across the suture and the periodontal ligament reorganizes. In RPE this is typically 4–6 months. In MARPE/MSE it is often 6+ months
- Bite adjustment — widening the upper jaw changes how the upper and lower teeth fit together. A short course of selective occlusal adjustment, a transitional splint, or orthodontic alignment usually follows
- Downstream treatment — expansion is often the foundation for what comes next: oral appliances for TMJ, sleep apnea appliances, or orthodontic alignment
- Re-evaluation — the airway, sleep symptoms, tongue posture, and jaw comfort are reassessed once retention is complete to see what (if anything) still needs to be addressed
Schedule a consultation if you'd like to find out whether expansion is the missing step in your TMJ, sleep, or orthodontic plan.
Dr. Cruz's clinical note
"I see palate expansion as foundational. Many of my TMJ and sleep patients have spent years stacking treatments — night guards, oral appliances, even CPAP — on top of an arch that is structurally too narrow to support the result they want. A high-vaulted palate, a crossbite, or a scalloped tongue is a clue that the architecture itself is the problem, and that no amount of soft-tissue or muscle work is going to fully solve it."
"For children and adolescents this is straightforward — the suture is open and the response is predictable. For adults, MARPE and MSE have genuinely changed what is possible without surgery. I will always be honest about which patients are good candidates and which need a SARPE referral — and I work alongside the right orthodontic and surgical specialists when the case is bigger than general dentistry can carry."
— Dr. Yolanda Cruz, DDS, Dr. Yolanda Cruz Dentistry On The Path, Downtown Toronto
Risks & considerations
- Palate expansion is a months-long commitment — the appliance must be worn consistently, and skipping retention is the most common reason for relapse
- Speech and chewing feel different for the first 1–2 weeks; this almost always settles as the tongue adapts
- A temporary midline diastema (gap between the upper front teeth) is normal during active RPE and closes during retention or with subsequent alignment
- Activation produces transient pressure across the nose and cheekbones; mild headache or facial soreness for a day or two is common
- In adults treated with conventional tooth-borne expanders, expansion may be largely dentoalveolar (tooth-tipping) rather than skeletal — results may be limited compared to MARPE/MSE
- MARPE/MSE involves temporary anchorage devices placed in the palatal bone; risks include mini-implant loosening, soft-tissue irritation, and rarely the need to reposition an implant
- Severe transverse deficiency in adults may not respond to MARPE/MSE and may need surgical (SARPE) management — this is an oral & maxillofacial surgery referral, not a general-dentistry procedure
- Outcomes vary with skeletal maturity, anatomy, compliance, and the presence of co-existing airway, periodontal, or TMD conditions
Frequently asked questions about palate expansion
Yes — in many cases. The midpalatal suture is fused in adults, so a conventional tooth-borne expander tends to tip the teeth outward rather than widen bone. Modern bone-borne appliances — MARPE (mini-implant-assisted rapid palatal expander) and MSE (maxillary skeletal expander) — place small temporary anchorage devices into the palatal bone and apply force directly to the skeleton. In appropriate candidates this produces genuine skeletal expansion non-surgically. When MARPE/MSE cannot open the suture, the alternative is SARPE — a surgical procedure performed by an oral and maxillofacial surgeon, which Dr. Cruz will refer you for if needed.
Coverage varies by plan and by what the expansion is being used to treat. When expansion is part of orthodontic care, many Canadian extended-health and dental plans contribute under the orthodontic benefit. When it is part of sleep-disordered breathing or TMD care, some plans contribute under medical or dental coverage; pre-authorization with documentation is usually required. Diagnostic imaging (CBCT) and the consultation are typically billed separately. We provide documentation for pre-authorization wherever possible. See the CDCP page for federal-plan eligibility.
The active expansion phase ranges from a few weeks (RPE in growing children) to several months (slow expansion or MARPE/MSE in adults). Retention — wearing the appliance passively while bone fills in — is at least as long again, usually 4–6 months for RPE and 6+ months for MARPE/MSE. Plan for the full process to span roughly 6–12 months from appliance delivery to the end of retention, with downstream orthodontic or appliance work potentially following.
For appropriately selected patients — particularly children and adolescents with maxillary transverse deficiency, and adults with a high-arched palate and narrow nasal airway — expansion can meaningfully widen the nasal airway and improve tongue posture, both of which support better breathing during sleep. It is not a guaranteed cure for obstructive sleep apnea in adults, and it is usually one part of a broader plan that also includes oral appliance therapy, ENT input, and sleep-medicine follow-up. A sleep study is the right way to measure whether the airway change has translated into a clinical improvement.
No — a midline diastema during active rapid expansion is normal and expected, especially in growing patients. It is a visible sign that the midpalatal suture is opening as intended. The gap typically closes on its own during the retention phase, or is closed with subsequent orthodontic alignment.
The practice is at 390 Bay St., Concourse Level, Unit C006 — on the PATH at the corner of Bay & Queen, downtown Toronto. The TTC Queen station is one block away and there's underground parking nearby. Full directions and accessibility notes are on the parking & directions page.
Medical Disclaimer
This content is for informational purposes only and does not constitute dental or medical advice, diagnosis, or treatment. Palate expansion outcomes depend on skeletal maturity, anatomy, compliance, and the presence of co-existing airway, periodontal, or TMD conditions. Some cases require referral to an orthodontic specialist, an ENT, a sleep-medicine physician, or an oral and maxillofacial surgeon. Consult Dr. Yolanda Cruz or another qualified dental professional regarding your symptoms and treatment options. Individual results may vary.
Ready to find out if palate expansion is right for you?
Book a focused consultation with Dr. Cruz in downtown Toronto. You'll leave with a working diagnosis, an honest answer about your candidacy, and a written plan — with no commitment to treatment on day one.